Relevance of the problem
Dermatomycoses (fungal diseases) constitute a large group of diseases of the skin and mucous membranes caused by the introduction and vital functions of plant microorganisms - fungi.
Dermatomycoses are of great interest because of the variety of pathogens and the clinical picture they cause, but mainly because of their tendency to spread, due to the high infectivity of the pathogens. The mushrooms belong to the class of the lowest plants without chlorophyll and unable to assimilate carbon dioxide. They are widely distributed in nature, which is explained by the conditions of their existence as parasites, opportunistic fungi and saprophytes. The mushrooms belong to a separate kingdom of Fungi, or Myceta (mushrooms), one of the 5 kingdoms of eukaryo. The kingdom of Fungi belongs to 4 departments:
- chitridiomyceta, which numbers 800 species that do not cause mycosis;
- zygomyceta has about 1000 species that cause mycosis and endomofluorosis;
- Ascomymyceta department includes 32 thousand species with sexual (reproductive) stage of life cycle and about 14 thousand species with vegetative (extra-sexual) stage. Ascomymyceta hyphae have a double-layered cell membrane, partitions, and the sexual stage is represented by an ascom (bag or bag) filled with spores. Ascomacetes are the agents of most mycoses;
- There are about 15 thousand species of Basidomyceta (basidomycetes). They have a sexual reproduction stage (spores) and a vegetative stage. Basidomycetes are the agents of cryptococcosis, multicolored deprivation and other Malassezia infections, white piedra and trichosponosis.
Under the name of dermatomycetes or dermatophytes (from the Greek word derma - skin, mykes - mushroom, phyton - plant), a special place belongs to the pathogenic fungi belonging to the lowest fungi - hyphomycetes - filamentous fungi, characterized by thread and spore formation; a significant part of dermatomycetes belongs to the class Ascomycetes. A common characteristic of dermatomycetes is their parasitization in the skin or its appendages - hair, nails. The source of infection with fungal diseases is a sick person, as well as sick animals. Infection occurs through direct contact with the sick, as well as through objects that were in contact with them and infected with fungi.
Getting into the body of a person or animal with hair and scales in the external environment, the mushrooms can show their vitality and virulence for a long time lasting for years.
The fungus gets to the surface of the skin and leads to its introduction into the stratum corneum. The latter is facilitated in the presence of maceration and micro-injuries, as well as the fact that the stratum corneum is not only a favorable nutritional environment, but also an optimal environment for parasitic fungi. Some types of mushrooms limit their location in the skin exclusively to the stratum corneum. Other mushrooms, such as microsporum and trichophytes, also affect the skin appendages - hair follicles, hair and nails.
According to the place of localization of the introduced fungi and the degree of inflammatory reaction, we can distinguish between surface and deep (subcutaneous) dermatomycoses.
The pathogenic impact of the fungus is not limited to the skin with its appendages. Chernogubov N.A. and Pelevin I.O. describe cases of universal skin lesions and gastrointestinal tract of fungal etiology. The vast majority of fungal diseases have a high degree of infectiousness. Of particular importance in epidemiological terms are trichophytosis, microsports, faunus, foot and hand mycosis, generalized mycosis and onychomycosis. The tendency of dermatomycoses to be widespread, especially among children, makes the problem of combating dermatomycosis especially urgent.
The importance of mycoses as a hospital-acquired infection has increased. The role of mycoses in transplantology, oncohematology, and neonatology is particularly significant. For example, Candida spp. Candida spp. displaces the hormonal excitatory bacteria. The group of mycoses firmly occupies a place in the structure of HIV-associated pathology. The growing importance of mycoses makes us improve the methods of their diagnosis and treatment, depending on the pathogens and forms of infection.
Brief historical information about fungal diseases
Fungal diseases have been known to mankind for a long time. Academician O.N. Podvysotskaya distinguished 3 periods in the history of our knowledge about fungal diseases.
The first period, the so-called descriptive, begins with deep antiquity (Hippocrates, Celsius) to the middle of the XIX century. The beginning of the study of mycoses in medicine dates back to the ancient era. Milkworm was described by Hippocrates and Galen, favaux (parsley) and infiltrative trichophytosis - Celsius, and the modern name of dermatophytosis (tinea) appeared in ancient Rome, when the first pathogens of fungal diseases were discovered. In 1842, the causative agent of surface trichophytosis and microsporia was described. In 1846 - the causative agent of multicolored deprivation.
The second period in the history of fungal diseases extends from half to the end of XIX century, which was facilitated by the invention of the microscope, the development of botany, and then mycology. During this period, were discovered new types of fungi: in 1839. - fungus is a pathogen of favaux, in 1842. - surface trichophytosis and microsporia, in 1846 - agents of multicolored deprivation, actinomycosis (1892) and blastomycosis (1894). The clinical picture they caused was studied and described, and the search for the most suitable nutrient media for the growth of fungi was carried out, thus initiating the study of fungal agents of all diseases in cultures (1899, Saburo). At the turn of the XIX-XX centuries. were described almost all the major mycoses of humans and their pathogens. Russian scientist Veryuzhsky was one of the first to prove that fungal diseases are caused by different fungi on the basis of numerous sowings of mushrooms in nutrient media. Proceedings of Veryuzhskiy were extremely important for solving the problem of etiology of fungal diseases and for complete defeat of unitary theory.
The third period stretches from the end of the XIX century to the present day. During this period, work on the study of toxins of fungi and immunity, as well as serology of fungal diseases, the issues of their treatment, the study of which led to an expansion of the arsenal of therapeutic agents.
The leading place in this period took our domestic dermatology, represented by such scientists as Pavlov S.T., Pospelov A.I., Nikolsky N.V., Friedman E.F., Bogrov S.L., Chernogubov N.A., Kartamyshev A.I., Bogolepov A.A., Podvysotskaya O.N., Araviysky A.N., Chubarova A.S., Arievich A.M., Kashkin P.N. and others.
Morphology of fungi
Mushrooms are plant organisms. Along with algae they are among the lowest plants and differ from the latter in that they do not contain chlorophyll and do not assimilate carbon.
The causative agents of pathogenic fungi (they are studied under a microscope) consist of threads of different lengths and thicknesses, called hyphae. Sometimes they are intertwined like felt. The intertwining of threads, or hyphae, makes up the mushroom's vegetative body and is called a mycelium or mushroom. The mycelium threads can be divided by transverse partitions into individual members (cells), as seen, for example, in mushrooms, which are the agents of trichophytosis, in this case mycelium is called septicaemia. In other cases, there may be no transverse septum - when the mycelium filament is represented as a single branched and sprawling cell resembling a hollow tube.
The mycelium filaments have a shell that consists of cellulose, fungin, chitin-like and acid-resistant substance. The shell of the mycelial thread contains fungal protoplasm, which consists of organic and inorganic substances. The protoplasm contains vacuoles and various inclusions: fat, glycogen, pigment, fibrous formations, crystals and resinous substances. The protoplasm of fungi contains cell nuclei in the form of small rounded formations of different sizes, in which the phenomena of mitosis and direct division by lacing the nucleus are observed. The chemical composition of the mushrooms is very diverse. It includes organic compounds - carbohydrates, proteins, fats, vegetable acids (oxalic, citric, acetic, ants, etc.), aromatic compounds, essential oils, alkaloids (muscarin, ergotine, etc.), glucosides, as well as inorganic compounds - salts of sodium, potassium, phosphorus, iron, sulfur, etc.. In addition, the vegetative bodies of mushrooms often contain pigment substances of complex chemical composition, giving the colonies of mushrooms purple, red, golden-yellow and other colors. The biochemical activity of fungi is characterized by their ability to release enzymes that break down proteins and fats, carbohydrates.
Depending on environmental conditions, in particular nutrition, mycelium of mushrooms can have a variety of forms. In some cases, the mycelium threads form constrictions that make them similar to the stems of reeds. Some mushrooms have mycelium endings in the form of short and thick branches and resemble candelabra or form interlacing similar to the antlers of a reindeer. These forms of mycelium are found mainly in pure cultures. The mycelium found in the pathogenic material appears more monotonous. In addition to detection of mycelium in laboratory diagnostics, the most important are spores, which, by definition, are acades. O.N. Podvysotskaya and Prof. P.N. Kashkin, are "lumps of condensed protoplasm, encased in a more dense and sharply contoured, sometimes double shell", i.e. morphologically, spores are formations that have arisen in the mycelium threads and separated from them - these are cells of reproduction of fungi, which are at the same time one of the stages of the existence of fungi and maintenance of their biological genus.
Pathogenic fungi are multiplied by spores, which, being more stable than mycelial threads, are formed mainly under unfavorable conditions for the development of mushroom life. Even after a long period of time, spores, once in favorable conditions, can germinate and form a new mycelium.
Agents of fungal diseases; are organisms that are in constant and close contact with the environment, assimilate the substances necessary for their lives. The latter are primarily carbon, nitrogen and mineral salts.
Proteins and carbohydrates are of great importance for the growth and vital functions of mushrooms. The reproduction of carbohydrates provides the mushrooms need for carbon. Of carbohydrates, glucose, maltose, levuleus, etc. are the most easily digested by the mushrooms. Nitrogen of the mushrooms is absorbed from peptones and amino acids, as well as from ammonium salts. From inorganic substances, the mushrooms need salts of potassium, iron, manganese, phosphorus, etc. for their nutrition.
The assimilation of nutrients by mushrooms is connected with their enzymatic activity. Most pathogenic fungi are able to produce enzymes that destroy tissue elements. Of these, proteolytic enzymes are particularly important, in particular diastase, which converts proteins into peptones, as well as lipase, emulsifying and washing fats. Lipase also plays an important role in the pathogenesis of dermatomycosis, dissolving skin fat and facilitating the penetration of fungi into the skin. The reaction of the environment is also important for the growth and development of fungi. Still Veryuzhskiy in his works showed that colonies of mushrooms grow best with a slightly acidic reaction of the medium. However, the boundaries of acidity of the medium in which the mushrooms can grow, fluctuate quite widely. Life cycle of mushrooms consists of two phases or stages: sexual (reproductive) and sexless (vegetative). The sexual stage of the mushroom's life cycle is called a teleomorphosis, while the anamorphous stage is called a no-sex phase. Another growth option is kidneys when a daughter cell is separated from her mother cell. In the reproductive phase, the body of the fungus has a complex structure and consists of differentiated cells with special reproductive organs. Among them, there are the structures of experience that allow you to endure unfavorable conditions. The mushrooms reproduce with the help of spores. The spores are formed as a result of simple mitosis and meiosis. In the first case, the type of spore formation and the stage of fungus development are called sexless, and the sexless spores themselves are called conidia. In the second case, the type of reproduction is called sexless, and the very name "spores" is more often applied to sexual disputes. Many mold fungus are characterized by the presence of special organs of conidiogenesis (sexless reproduction). The budding daughter cells of yeast fungi are called blastoconidia.
Resistance of mushrooms
We can assume that the temperature limits of mushroom growth vary between 15° and 50° above zero. The most favorable temperature for the growth of mushrooms is 25-30 ° above zero.
According to A.M. Arievich, P.N. Kashkin and other authors, sunlight delays the growth of dermatophytes, so daily for one hour sunlight illumination of mushrooms leads to the death of mushrooms, both in cultures and in pathological material.
The resistance of dermatophytes to chemicals is quite high. It is known that after 10-minute exposure to formalin (2%), bicarbonate soda (10%), carbolic acid (2.5%), when exposed for a few seconds to a solution of chlorine lime (0.5%), fungus death is observed. Iodine tincture (10%), aniline paints - fucorcine, methyl-violet, diamond greens (1-2%), salicylic and benzoic acid (1%) have the same effective effect.
In the pathological material, especially in the hair, mushrooms can keep their vitality for a long time. Academician O.N. Podvysotskaya indicates that fungi in the hair retain their pathological properties for one year, and in nail plates and scales - from 4 weeks to six months. There are separate indications of the viability of pathogenic fungi during 3-8 years (Itkin, Malyshev).
Studies show that the viability of mushrooms is due to the presence of spores resistant to external influences, while mycelias are dead. This resistance to spores in the pathological material is an extremely important epidemiological factor. The existing division of fungi into saprophytes and opportunistic mushrooms seems to be extremely conditional. Therefore, it is necessary to identify important pathogenetic factors that contribute to the transition of these fungi into a pathogenic or, one might say, parasitic state:
- hypoavitaminosis,
- endocrinopathy, especially diabetes mellitus,
- Dysbacteriosis and other gastrointestinal diseases,
- immune deficiency status, in particular HIV infection.
Methods of diagnostics of fungal diseases
1. Microscopic examination is the most convenient and common method of examination for fungi. To obtain reliable results of the study for mushrooms, it is recommended to take the material before treatment. The material for the study is taken from peripheral places, representing the freshest centers of lesions. Flakes, hair and nails are more or less dense opaque horn matter and therefore should be treated accordingly before microscopic examination. Only as a result of the treatment of the pathological material is its separation with the release of fungi contained in the cornea tissues, and the clarification of the latter. Therefore, conditions favorable for the detection of mushrooms are created. The best reagent for enlightenment is 30% solution of caustic potassium or sodium. Flakes and nails should be broken down into small particles. Hair is cut into the smallest transverse segments. Microscopic examination of pathological material is the most convenient and common method of examination for fungi. A characteristic feature of the elements of fungi is the increased light refractibility, allowing them to distinguish well from other microscopic formations.
Mycelium of fungi is found in the preparation in the form of long, twisting, branching threads. It is often possible to see the division of mycelium into members (septicaemia) of different lengths and widths. Mycelium in form and structure seems peculiar, which is not difficult to differentiate from other formations with a slight skill. Discovery of only one strand of mycelium in the drug allows in many cases to confirm the clinical diagnosis of fungal disease. This is more difficult to do when only spores are detected in the drug, especially in cases of their atypical location. In the flakes and nail particles, fungi are found in the form of branched mycelium and spores, arranged in a chain. In this case, it is not possible to determine the type of mushroom in the vast majority of cases, as different types of mushrooms can give the same microscopic picture. If there are very short mycelium strands in the preparation, it is possible to assume the presence of a microsporia pathogen with a known degree of probability. Guided by the size of spores, we can also talk about large- and small-spore trichophytosis and microsporia.
From all this it should be concluded that in the study of scales and nail particles, the diagnosis of fungal disease is made on the basis of the discovery of mycelium or spores of fungi. The laboratory response should indicate whether or not fungi have been detected.
In the microscopic examination of hair, it is very important to determine the fungus' attitude towards it. The elements of the fungus - mycelium and spores - can be located both on the surface of the hair (ectotrix type) and inside it (endotrix type). In the first case, the elements of the fungus, located on the surface of the hair, may penetrate in smaller amounts inside it. A distinction is made between large-spore and small-spore ectotrix by the size of spores. When small spores are detected on the surface of the hair, covering it for some time like a cover, the question arises about the difference between the finely sporied surface trichophythy and microsporia. In surface trichophytosis spores have the same size and shape, they are arranged in chains along the length of the hair. In microsporia spores are arranged without any system, like a mosaic. Mycelium and fungal spores can be located inside the hair (endotrix type). Often the microscopic pattern resembles a bag of nuts. The role of the latter is played by spores arranged in chains along the length of the hair (Trichophyton endothrix). The fungus, the faunus causative agent, is also located inside the hair, but its elements, unlike the trichophytosis, never fill the whole hair substance and leave part of it unchanged. The mycelium threads predominate and little spore in the hair is detected. In addition, the hair affected by the faunus contains air bubbles.
Thus, the microscopic study of hair reveals the fungus relation to the hair, the location of the fungus outside or inside the hair, the size, shape and grouping of the fungus elements. A more precise, comprehensive answer can only be given through a cultural study.

2. Cultural study of mushrooms. Cultivation of mushrooms on artificial nutrient media is a widely used method of mushroom study. The vast majority of nutrient media contains carbohydrates and peptone, the ratio of which varies in a fairly wide range of sizes in different media. Medium Saburo (sugar agar). It consists of maltose (glucose) 4.0; peptone 1.0; agar-agar 1.8; distilled water - 100 cmS. Saburo's environment enjoys wide popularity and distribution. It gives good growth of mushrooms, is relatively easy to prepare and does not require complex devices for its preparation. Growing mushrooms on nutrient media is a common research method to ensure the correct diagnosis of fungal diseases, determining the type of fungal pathogens, as well as the choice of effective treatment methods and preventive measures. The optimal reaction of the nutrient medium for growing most dermatophytes is weakly acidic, it ranges from pH - 6.0-6.8. The most favorable temperature conditions for the growth of fungi in the thermostat varies between 25 and 28 degrees above zero.
The appearance of crops depending on the type of mushrooms is very diverse. Pathogenic fungi, depending on the released pigment can color the colonies in different colors. Violet trichophyton (Trichophyton violaceum) - a causative agent of surface trichophytosis - got its name from the characteristic reddish-purple pigment, which stains its colony. Besides, the culture of purple trichophyton has the form of dome-shaped elevation of rounded outlines, the surface of cultures is matte, less often it appears oily and covered with folds.
Pathogens of superficial yeast dermatoses (Candida), fungi of the genus Candida, give colonies of various shapes and kinds, have a smell of yeast. Their type is determined by the ability to cause the fermentation of this or that kind of sugar.
Dermatophytoses
Skin mycoses caused by mycelial and yeastlike fungi are called dermatomycosis.
Nail mycoses caused by mycelial and yeastlike fungi are called onychomycosis.
Mycoses of the skin and its keratin-containing appendages caused by dermatophytes are called dermatophytosis or dermatophytosis.
Dermatomycosis and onychomycosis, except for dermatophytes, may be caused by the following fungi:
Dermatomycoses
- Candida spp.
- Fusarium moniliforme
- Trichosporon beigelii
- Hendersonula toruloidea
Onyhomycosis
- Scopulariopsis brevicaulis
- Acremonium sp.
- Aspergillus flavus, A. fumigatus, A. glaucus, A. teereus, A. versicolor
- Fusarium oxysporum
- Geotrichum candidum
- Candida albicans
- Hendersonula toruloidea
- Cephalosporium sp.
Dermatophytoses (English synonyms "tinea" or "ringworm") are the most common surface mycoses of humans and animals, which affect the keratinous tissue of the skin, hair and nails. They are caused by a group of related mycelial keratinophilus fungi, commonly called 'dermatophytes', which are able to use keratin as a food source. This group includes about 100 mushrooms, most of which are soil keratinophilous mushrooms, but only 42 species are recognized as authentically existing and are really associated with human mycoses. Of these, 11 species are most common as agents of dermatophytosis. It is assumed that in the process of evolution, soil fungi have adapted to certain hosts and gradually formed the existing groups of anthropo, zoo- and geophilic dermatophytes.
Imperfect forms of dermatophytes are divided into 3 genera:
- Epidermophyton genus - produces only macroconidia in the absence of microconidia. It includes 2 species, one of which is pathogenic to humans.
- Microsporam -produces microconidia and Shorehovy macroconidia. Described 19 species, of which 9 cause infections in humans and animals.
- Trichophyton genus - produces smooth wall macroconidia and microconidia. Includes 22 species, mainly causing infections of humans and animals. Perfect forms belong to the genus Arthroderma gymnoscopic.
About 60% of all species separated from humans are T. rubrum, about 25% T. mentagrophytes, about 10% - T. verruco-sum and T. tonsurans. All other species: E. fioccosum, M. ionini, M. canis and others - causes 1%-5% of all dermatophytosis.
Sources of infection and epidemiology
Dermatophytes are the only group of really contagious mushrooms, i.e., able to transmit from one living source (people, animals) to another.
The prevailing species of dermatophytes, which cause skin mycoses, differ in different areas.
Dermatophytes are divided into natural reservoirs and sources of infection for humans:
- anthropophiles, which are found almost exclusively in humans, cause predominantly mild, chronic infections;
- zoophytes are typical for domestic and wild animals and birds. In humans, they cause island-inflammatory and rapidly expiring infections;
- Geophilic dermatophytes, which have their own reservoir of soil, cause island-specific limited infections, usually spontaneously curable.
Dermatophytoses are found all over the world, and their frequency, localization and prevalence depend on environmental factors, lifestyle and customs of the population.
Dermatophytosis species such as T. Mentagrophytes, T. Rubrum, E. floccosan
Some types of dermatophytes have limited geographical distribution and are endemic in certain areas. Thus T. soudaneuse, T. gourvilii and T. yaoundi are geographically limited to Central and West Africa. M. Feirugineum is mainly distributed in Japan and its surrounding areas, T. Yaoundi is registered in the South Pacific, in Central and South America.
However, increasing population mobility leads to changes in the range of dermatophytes distribution. For example, T. tonsurans has displaced M. audouinii as the main pathogen of scalp mycosis in the USA due to intensive migration from Mexico and other South American countries where T. tonsurans dominates.
Dermatophytes are spread by direct direct contact with an infected source (human, animal, soil) or by indirect contact through infected skin or hair scales (combs, clothes, shoes, furniture, theater chairs, hats, bedding, towels, carpets).
Depending on the type of dermatophytes may remain viable on the objects of the environment up to 15 months.
Dermatophytosis pathogenesis
Dermatophytes colonize keratinous tissues and in response to their cells and metabolites, an inflammatory reaction occurs at skin level. Lesions are mainly skin-based due to the inability of dermatophytes to invade deep tissues and organs. Only in rare cases are subcutaneous tissues involved (kerion, Mioca granuloma) or a generalized systemic infection caused by dermatophytes occurs.
In vitro dermatophytes damage keratin by a combination of enzymatic digestion by proteins (keratinases) and mechanical pressure.
In vivo, their activity is manifested in the differentiation zone on newly synthesized keratin. During the incubation period, the hyphae grow into the stratum corneum of the skin and then into the hair follicles and the hair shaft, affecting the new follicles.
To maintain infection, the fungus growth is coordinated with the speed of keratin production. The infection process stops and the healing begins when the newly synthesized healthy keratin removes the fungus hyphae from the keratinized zone.
Trichoplyton species affect the skin, hair and nails. Microsporum genus species affect the hair, skin and very rarely nails. Epidermophyton species affect the skin and nails, but not the hair.
They are predisposed to infection: hereditary factors, microcirculation disorders, fever, humidity.
Diseases begin with local inflammation at the site of the initial introduction of the fungus. Inflammatory changes are most pronounced at the peripheral border of the foci.
Clinical manifestations of diseases are classified according to the anatomical localization.
Laboratory diagnostics
The diagnosis of dermatomycosis is made on the basis of the clinical picture and the results of laboratory tests.
Laboratory tests consist of the following steps:
- Taking and transportation of pathological material;
- Material microscopy;
- Selection and identification of pure culture of the pathogen with the determination of sensitivity to chemical preparations;
- Serological and allergic studies.
Taking and transportation of pathological material
The correct taking of the material significantly affects the success of microscopy and culture, as not all scales and hair from the lesions contain elements of the fungus. Pathological material should be taken as much as possible from foci that have not been treated locally.
Skin scales are scraped from the active peripheral edges of the lesion area or at the interfinger intervals using a sterile, slightly blunted scalpel. Fragments of the macerated, whitish horn layer and the tires of the bubbles are taken with tweezers. Surface crusts and scales in the center of mycotic centers contain much less mushroom elements and are less suitable for research. The day of taking the material from peeling hearths on smooth skin and in children can be used transparent adhesive tape.
Deep layers of the affected nail plate are scraped off with a scalpel, removing loose horny masses. To take the material from the affected nails use nail scissors, scalpels, tweezers, dissecting needles. Obtaining finely chopped pathological material facilitates further research.
When the hair is affected with epilation tweezers remove the deformed, whitish, broken hair at the periphery of the focus, changed color and lost elasticity.
Voodoo Lamp Study
The Vooda lamp is a tool to facilitate the diagnosis and taking of the material under study in the clinical and subclinical forms of fungal infections and is also used to control cure. The Vooda lamp is an ultraviolet lamp with a glass filter consisting of barium silicate with 9% nickel oxide and long wavelength UV rays of 365 nm, used for irradiation in the dark from a distance of 20 cm to the surface. The Vooda lamp causes fluorescence induced in some microorganisms.
Bright green fluorescence is observed when hair is affected by dermatophytes of the genus Microsporum (M. audouinii, M. canis, M. ferrugenium, Mdistortum). The method allows quick and easy screening of large groups of people (children) in case of microsporum suspicion. Limits the use of Voodoo lamp to increase the etiological role of T. tonsurans (weak fluorescence) and other non-fluorescent dermatophytes.
In case of multicolored lichen (M. furfur) the affected skin has golden-yellow fluorescence, in case of erythrazm (causative agent -Corynebacterium minutissimum) - red, in case of wounds affected by bacteria of the genus Pseudomonas - bright green. The artifacts in the study may be due to the use of some cosmetic and antifungal ointments.
Sterile corduroy, a carpet flap, a sterile hand washing brush with a bandage stretched on its nap to a depth of 0.3-0.5 mm, which creates a filter-like layer on which scales and hair are trapped when combing the hair. For sowing, the bandage is spread on the nutrient medium until the growth of the fungus.
Pathological material can be collected in sterile Petri dishes; between two sterile object glasses, bound with elastic bands and wrapped in paper; in black paper bags to better see flakes and hairs. The use of parchment and wax paper should be avoided, as the loss and spread of pathogenic material may occur when unfolding.
Transportation and shipment of material is carried out in sterile boxes with accompanying documents. Accompanying paper should be specified:
- Full name, age and sex of the patient;
- institution and name of the doctor;
- date of taking and nature of the material;
- the expected diagnosis and medical history number.
For taking and examination of the material it is desirable to have the following equipment: light microscope, phase-contrast device, illuminator, ocular micrometer, mycological blades, bacteriological loops, dissecting needles, scalpels, epilation tweezers, surgical and anatomic tweezers, scissors, spatulas, gas burners or distilleries, Petri dishes, slide and cover glasses, bacteriological tubes, centrifuge tubes, slide glass with holes, flasks, funnels, pipettes measuring, eye, pastries, glass sticks, pencils on glass, magnifying glass.
Work in the mycological laboratory related to the study of infectious material should be carried out in accordance with existing instructions on safety and antiepidemic regime. The laboratory should have cabinets for clean dishes, tools, nutrients and reagents. For disinfection of working tables, glasses with pathological material, protective cages use 5 % chloramine solution, lysol solution and other means specified in the Instruction of the Ministry of Health of the USSR № 985-72 on carrying out antiepidemic and disinfection measures at microsporia, trichophytosis and favaux. Tools and dishes are subject to decontamination and thorough mechanical cleaning after use when taking the material. Mushroom cultures and pathological material are autoclaved for 30 minutes at 120° or boiled for one hour. Desks and air in the laboratory are sterilized with UV light from a mercury quartz lamp.
Pathological material is examined as soon as possible after it is taken. To do this, it should be divided into 3 parts:
- for microscopy;
- for obtaining cultures;
- for repeated control examination.
Pathological material microscopy
The easiest and fastest method to establish the presence of fungus in tissues. For this purpose, the skin and nail scales are crushed by dissecting needles, and long hair (in favaux) is divided into short fragments (0.1-1 mm) by the rib of a heated scalpel or calcined with a dissecting needle. Grinded material is placed in the middle of the slide glass, apply 1-2 drops of 10% KON and slightly heated over the flame until the appearance of a whitish rim on the edge of the drop, not bringing to a boil, cover with cover glass and leave for 5-10 minutes (hair, skin scales), 30-40 minutes (nail scales) for maceration and enlightenment.
If the product is overheated, pressed or treated for too long, the hair is deformed and the spores and mycelium of the fungus are disturbed. To avoid heating, the preparation is kept in 20% KON 30-60 minutes. The preparations are first microscoped at low magnification with the condenser lowered or with the aperture diaphragm covered to obscure the field of view; then the selected places are viewed at high magnification of the dry system with the condenser raised. If there are few fungus elements (at the beginning of the disease) or if they are blurred, it is recommended to use a phase-contrast device.
In addition to the KON, there are a number of solutions used to clarify the keratin of cornflakes and hair: lactofenol (20 g 85% lactic acid, 40 g of glycerin, 20 ml of distilled water, 20 g of crystal carbolic acid and 0.05 g of cotton blue), chlorlactophenol (20 g of crystal chloral hydrate, 10 g of crystal carbolic acid, 10 g of lactic acid), 10% aqueous-alcohol solution of sodium sulfide, 15% KOH in 15% dimethyl sulfoxide on distilled water. Optimal and approximately equivalent solutions clarifying skin and nail scales are 10 % KON, 15 % KON+15 % DMSO and 10 % Na2S.
For the treatment of rough horny masses of nails, skin scales from the soles and palms and during mass inspections, enrichment methods are used. The material in centrifuge tubes is poured 1.5-2 ml 20% KON, boiled in a water bath for 30-60 minutes, then centrifuge for 15 minutes at 3000 rpm or stand for 1 day. After draining the liquid, the sludge is transferred to the slide glass with a pipette and microscoped.
It is recommended to treat nail scales with PAS (periodic acid-Shiff) method, which stains the mushroom hyphae in red.
The nature of the dermatophytes lesions in the hair allows us to determine the genus of the fungus. The species can only be determined by culture.
There are the following types of hair affection with dermatophytes:
- Trichophyton ectotrix - Arthrospores are placed in wrong chains outside the hair, surrounding it at the base. Affected hair does not fluorescence. Tr. ectotrix has two varieties: Tg. ectotrix megasporon (large-spore, spore size 8-12 microns), is characteristic of the defeat of T. equinum, T. gallinae, T. megninii, T. rubrum, T. verrucosum and Tr. ectotrix microides (small-spore, spore size 3-5 microns), is characteristic of the defeat of T. mentagrophytes.
- Trichophyton endotrix - arthrospores 3-5 microns in parallel chains are located only inside the hair. The affected hair is not fluorescent: it curls and breaks, leaving short hemps or "black spots". This type of lesion is typical for T. tonsurans, T. violaceum, and also for African dermatophytes T. gourvilii, T. soudanense, T. yaoundei.
- Microsporum - arthrospores 2-3 microns in size (not clearly visible at low magnification) randomly mosaic inside the hair and a whitish cover surrounds the hair shaft from the outside. The affected hair fluoresces brightly; when broken, it leaves 5-8 mm hemp. This type of hair damage is typical for M. audouinii, M. canis, M. distortum, M. ferrugineum. When pressing on the cover glass in a preparation of microsporamic affected hair, sometimes you can see a micelial fringe - the so-called "Adamson brush". The hairs affected by M. gypseum, M. fulvum, M. nanum, M. vanbreuseghemii do not fluorescence; the spores are larger (5-8 microns) and are visible at low magnification.
- Trichophyton is a polymorphic lesion of hair typical for favus by septized mycelium hyphae of different width and arthrospores of different size located inside hair containing air bubbles and fat droplets. The hair is not filled with fungal elements, remains long; it is weakly fluorescent under a Vood lamp. However, the diagnosis should not be based only on the presence of air bubbles and fat droplets in the hair, as they are sometimes observed in other types of lesions. In addition to the Achorion type of hair lesion, the faunus is characterized by the formation of sculls, yellow crusts containing hyphae and spores of the fungus. This type of lesion is caused by T. schoenleinii, T. violaceum, M. gypseum.
In the flakes of smooth skin affected by dermatophytes, you can see hyphae of septized branch mycelium 2-4 microns wide, sometimes chains of rounded or polygonal arthrospores 4-7 microns in size. Chains or clusters of arthrospores and less often mycelium hyphae are more often observed in nail scales.
Should be distinguished from the elements of the fungus such artifacts arising in the preparations, as the so-called "mosaic fungus" (located on the borders of epithelial cells, consists of fragments of organic nature of different sizes), elongated crystals of alkali (polygonal form); disappear when washing the preparation, for which on the one hand, apply a drop of water, and on the other hand, place a piece of filter paper and be careful not to lose material, repeat 2-3 times, fat drops (different sizes, lack of internal structure), cotton threads (size, homogeneity, irregular shape, brush at the end).
In conclusion, the microscopy of the pathological material indicates the type of hair damage, the presence or absence of mycelium and spores of the fungus in the skin and nail scales. However, it is believed that the hyphae of dermatophytes in drugs are indistinguishable from mycelium of yeastlike or moldy fungi. Therefore, to determine the type of pathogen should be combined with a microscopy of the pathological material to obtain a pure culture. In this case, samples of pathological material should be cultivated in case of negative results of microscopy.
Cultural Research
It is necessary to isolate and identify the pathogen, to determine latent dermatophytosis, the carriage of dermatophytes by healthy individuals, to identify dermatophytes in the environment and to determine the sensitivity of the culture to chemotherapy.
Getting a clean culture
The investigated material should be as much as possible crushed and sown in minimum quantities on beveled agar in tubes at 2-4 points at a distance of 1-2 cm. The material of one sample is sown at least 2-3 tubes (hair) and 4-5 tubes (skin and nail scales) on two different nutrient media. For primary isolation of dermatophytes it is preferable to use a standard agarized medium Saburo (SDA); 2 or 4% glucose (glucose 20 or 40 g, peptone 10 g, agar 20 g, distilled water to 1000 ml, pH 6.8-7.0), agar must (beer must diluted with distilled water to 7% of carbohydrates by Balling, agar 20 g) or Saburo medium with antibiotics: antibacterial antibiotics (penicillin: 50 µg/ml + streptomycin 50-100 µg/ml or levomycetin 50 µg/ml or biomycin 200 units/ml, gentamicin) and antifungal antibiotic actidion (cycloheximide) 0.1-0.4 mg/ml. Preparation of selective media with antibiotics - 200 000 units of crystal penicillin is dissolved in 10 ml of sterile water, 1 ml of this solution + 9 ml of water give a concentration of 2000 µg/ml. Adding 2.5 ml of this dilution to 100 ml of melted and cooled to 50° medium gives a concentration of penicillin 50 µg/ml. The addition of streptomycin (1 g streptomycin=1 million units) to the medium is similarly performed. Biomycin is added by dissolving 1 tablet (100000 units) in 500 ml of cooling medium. Levomycin is preliminary dissolved in 10 ml of 70 ° ethyl alcohol and added to the medium to a concentration of 50 µg/ml. Actidione (Streptomyces griseus antibiotic) is a white crystalline powder, thermostable, well soluble in acetone. In 1 ml of acetone, 10-50 mg of actidion is dissolved, brought to 2 ml with distilled water and added to 100 ml of cooling medium. Actidione does not affect the growth of dermatophytes and suppresses many mold fungi, as well as species of Candida and Cryptococcus. Therefore, if there is a suspicion of the ethical role of these mushrooms should be sown also on environments without actidione.

Seeds are incubated in a thermostat at 25-30-37 °, respectively (more than 30 °) and studied weekly for up to 4 weeks. If suspected on T. verrucosum half of the sown tubes should be incubated at 37 °, because the fungus grows faster at this temperature. The first signs of growth of dermatophytes mark from 4 to 12 day incubation at the sowing points on the edges of the material. If no growth for 30 days, the results of cultivation are considered negative. In optimal conditions, the primary crops of many dermatophytes can be identified on 7-10 days after sowing, but in the case of faviform fungi sometimes only on 20-30 days. Primary crops grow relatively slowly and with media without antibiotics can be suppressed by faster growing bacteria and mold fungi. Unlike the latter, colonies of dermatophytes are never black, blue or green. It is important to observe asepsis when taking and storing the material, as well as to study it in the shortest possible time. When there is growth, it is desirable to make a sifting from the edge of the primary culture to the fresh environment to obtain a clean culture. Before incubation, seeded and labeled Petri dishes should be wrapped in polyethylene or paper to prevent rapid drying and secondary air pollution.
Identification of pure culture
Characteristics of colonies
When describing colonies should be noted such features as the time of appearance and growth rate of the colony, its size, color of the surface and backside, the nature of the surface and its topography, shape and edge of the colony, its consistency and the presence of ingrowth in the substrate. Characterizing the colony, indicate its differences from the typical strains, which is important for assessing the polymorphism of this fungus species, as well as to identify atypical strains and new, rare in Russia.
Microscopic study of cultures
With low magnification and strong light, you can explore the edge of the colony through the glass tube, as mycelium filaments move onto the glass. The presence and location of characteristic morphological elements (conidia, spirals) in combination with cultural features in some cases allow to determine the species without preparation of micropreparation or microculture. In this study, the tube can be fixed by hand or a wooden stand with a neckline can be used.
To prepare a microdrug, a fragment of culture is split with a mycological spatula and a dissecting needle on a slide glass in a drop of liquid (water, Lugol solution, lactofenol, ethanol+water 1:1, ethanol+glycerine + water 2:4:4) and covered with a cover glass. The culture for the study is taken from the central and peripheral zone of the colony. Microscopy should be done first under a small (*8) and then under a large (*40) magnification of the dry microscope system. The elements of the fungus are measured with the help of an ocular micrometer, the fission value of which is preliminary determined by the object-micrometer.
Microcultures are prepared to study the micromorphology of the fungus with the aim of "precise identification"
On the center of a cover glass the drop of the liquid environment containing mushroom elements is put, and it is established its drop down on greased Vaseline Vantihem ring or subject glass with a hole. A drop of water is added to the bottom to prevent it from drying out. It is possible to prepare microcultures in agar blocks. To do this, cut out of the agar squares 10x10 mm, 2 mm high and transfer them to the slide glass. The culture is sown in the middle of each edge of the agar square, covered with cover glass and the gap between cover and slide glass is filled with pre-melted wax to prevent it from drying out. The microcultures are incubated in a humid chamber (Petri dish or extractor with moist wool).
The microscopic characteristics of cultures should take into account mycelium septicaemia, the presence, nature and method of attachment of macroconidia and microconidia, as well as the structure of mycelium and its formations - spirals, scalloped hyphae, favicheskie candelabra. The presence and character of chlamydospor have no decisive diagnostic value.
Biochemical differential-diagnostic tests
If it is impossible to identify strains based only on their morphological features, tests are used to determine some manifestations of metabolic activity of fungi. For laboratory practice, methods to determine nutritional needs and methods to determine the enzymatic activity of dermatophytes have been developed.
Determination of nutritional needs and vitamins.
The basic minimal medium (NH4NO3 1.5 g, glucose 40 g; MgS04 - 7NgoO 0.5 g; KN2RS>4 1 g; agar Difko 20 g; distilled water up to 1000 ml) is dissolved at heating and autoclaved at 0.5 atm 15 min. Vitamins (thiamine 1 mg, i-inosite 250 mg, L-histidine 150 mg, nicotinic acid 10 mg) are dissolved in 100 ml of distilled water each, autoclave at 0.5 atm 15 min and keep in the refrigerator. Before the experiment, 2 ml of this or that vitamin is added to 100 ml of cooling main medium. To determine the ability to assimilate carbohydrates, they are added to the base medium instead of glucose to the final concentration of 1%. Sources of nitrogen nutrition is introduced into the medium instead of NH4NO3. Control are sowing in the basic and enriched media.
Keratinolytic activity (Hair Perforation Test).
A) Finely crushed cleaned soil is sterilized in an autoclave for 3 days in a row for 1 hour at 1 atm. and placed in Petri dishes with an even layer of 3-4 mm. On the surface of the soil evenly and not densely distributed cut into short fragments (15-20 mm) baby hair, sterilized in an autoclave 2 days in a row for 20 minutes at 1 atm. On the surface of the soil-hair medium a suspension of the studied crop in 1-2 ml of distilled water is applied. The crops are incubated for 4 weeks at 22-27° with weekly moistening of the medium with sterile distilled water. The presence of organs-perforators or other forms of keratinoli-zis is recorded by a weekly microscopy of the hair, which is the development of fungus culture.
B) A strip of filter paper is placed on the bottom of a sterile Petri dish and covered with sterile distilled water. The sliced sterilized hair, 5-6 drops of 1% yeast extract and suspension of the studied culture are brought in. Incubated at 25° for 4 weeks. Hair is microscoped weekly for the presence of conical organs - hair shaft perforators. This method is used to differentiate T. equinum, T. raentagrophytes, T. rubrum as well as to obtain perfect forms of dermatophytes from the soil.
Differential medium with milk, glucose and bromcresol - purple (HRV + CCG + 0.5% yeast extract) allows to differentiate the types of dermatophytes in two parameters: za-leaching medium (blue -> purple) and the zone of enlightenment around the colonies due to hydrolysis of milk.
Hemolytic activity is determined on the medium Saburo pH 6.5 with a phosphate buffer and 5% defibrinated lamb blood. Erythrocytes are brought into the cooled agar, and the medium is poured into cups with a thick enough layer. After sowing the cultures under study, the cups are incubated for 2 weeks at 27°. Hemolytic ability is judged by the formation of a zone of enlightenment around the colonies due to the dissolution of erythrocytes. The greenish coloring of this zone is considered to be alpha-hemolysis, the presence of a transparent and colorless zone - like beta - hemolysis. Control is provided by unsown cups with 5% of cro-h dried agar. The test can serve for differentiation of T. rubrum and T. mentagrophytes, as well as T. tonsurans and T. soudanense.
The determination of urease activity (ability to split urea) is done on Christensen's urea environment. Medium composition: peptone 1 g, NaCl 5 g, KN2PO4 2 g, glucose 5 g, agar 20 g, distilled water to 1000 g. The ingredients of the medium are dissolved when heated, pH is brought to 6.8 and 6 ml 0.2% solution of phenol red is added (0.2 g phenolrot is dissolved in 20 ml of heated ethanol and 80 ml of heated distilled water is added). Sterilize the medium 20 min at 0.5 atm, cool it down to 50° and add 100 ml of aqueous urea solution (sterilized through a bacterial filter or 15 min at 0.5 atm). Pour the medium in tubes, mow and incubate for 7 days at 25°-30°. The results are assessed by the presence and timing of red coloring of the medium, which is an indicator of urease activity of crops. Unseeded test tubes with the medium serve as a control. The test is used to differentiate atypical strains of T. rubrum and T. mentagrophytes, as well as to identify T. gallinae, "African" trichophytons and some species of Microsporum.
Determination of the temperature optimum
Incubation of parallel crops at t 25 °-30 °-37 ° on the beveled agar Saburo. Used for differentiation of T. men-tagrophytes and T. terrestre as well as T. verrucosum and T. schonleinii.
Serological and allergic studies
Serological tests: Precipitation reaction in the variant of immunodiffusion in agar gel
Patient's serum is introduced into the central hole made in agar gel, and antigens of cultures of different species are introduced into the surrounding holes. The results are taken into account after 48 and 72 hours of incubation at room temperature and then after 2-3 days in the refrigerator. To check the specificity of precipitation lines, a drop of 1.5% EDTA is added to the central well and after 1 hour non-specific precipitation lines disappear.
Allergic tests: intracutaneous tests with trichophytin, an active component of which is galactomannan-peptide
The carbohydrate component detects an immediate type of allergy (GNT), while the protein component is associated with the detection of cellular immunity (CVI). Patients who do not exhibit GHT or give GHT often have a chronic form of dermatophytosis.
Characterization and differentiation of the main dermatophytosis pathogens
E. floccosum (synonyms of E. inguinale, E. cruris).
Anthropophilus. Affects the skin of inguinal folds, shins, interfinger folds of feet, nails.
Primary crops develop on 4-5 days. Colonies folded, domed, mealy. The color of the colony is yellow with a greenish tint, the reverse side of yellow to brown.
At microscopy of culture numerous thin and smooth-walled, obtuse-tipped macroconidia with 2-6 partitions, single or 2-8 in the form of bunches of bananas are visible. There are no microconidia. When cultures age, chlamydospores and art spores appear. The minimum inhibitory concentration of griseofulvi-na, inhibiting the growth of E. floccosum cultures, is 1 mkg/ml.
Microsporum genus.
M. audouinii. Anthropophilus. Affects the scalp fluorescence of children's hair and smooth skin.
Primary crops develop on 6-8 days. Colonies are slow growing, flat, fluffy, with radial folds. The surface is white to cream, the back side is yellowish brown. In microscopy, rare bumpy, thick-walled macroconidia and polymorphic microconidia are visible.
In old cultures, there are numerous chlamydospores. The growth of fungus stimulates the addition of nicotinic acid to the environment. The minimum inhibitory concentration of griseofulvin is 1 mg/ml.
The fungus can be distinguished from similar cultures of M. canis by its weak growth on polished rice, the lack of ability to hydrolyzoate gelatin and use urea, NH4NO3 and trehalose as the only sources of nitrogen and carbon nutrition.
M. canis (synonyms of M. lanosum, M. felineum). Zoophilic der-matophyte (cats, dogs). Affects the scalp fluorescence in children, smooth skin and fluffy hair.
Primary crops develop on 5-10 days. Colonies of eugonic strains are fast growing, flat, fluffy. The color of the surface is gray to cream, the back side is yellow orange. Dysgonic strains are leathery, elevated and pigmented. Numerous spindle-like, pointed macroconidia with bumpy and thick wall (2 microns), consisting of 3-15 cells, can be seen during microscopy. Microconidia are found.
In old cultures, there are numerous chlamydospores. According to our data, 94% of strains have MIC 5 µg/ml, and individual strains are suppressed with only 7.5 and 20 µg/ml of grizeofulvin.
The fungus can be distinguished from similar cultures of M. audouinii by its good growth on polished rice grains, ability to hydrolyze gelatin and use urea, NH4NO3 and trehalose as the only sources of nitrogen and carbon nutrition, as well as the presence of a perfect form of Nannizziae otae.
M. ferrugineum (synonymous with T. ferrugineum). Anthropophilus. Affects the scalp fluorescence in children with fluorescence of hair and less often smooth skin. Primary crops develop on day 8-10. Colonies are slow growing, folded, leathery and waxy, sometimes velvety. The color of the surface and back is orange.
In microscopy of cultures can be seen: bamboo mycelium, scalloped hyphae, deer horns, arthrospor chains, an abundance of chlamydospor. There are no conidia. The minimum inhibitory concentration of griseofulvin is 5 µg/ml.
It should be distinguished from similar cultures of T. schoenleinii by the type of hair lesion and its fluorescence, by its ability to absorb trehalose and inability to absorb urea. T. verrucosum differs from the cultures by the fluorescence of the affected hair, pigmentation of colonies and the lack of vitamins. From similar cultures T. soudanense differs in the type of hair lesion and its fluorescence, colorless colonies on the rice medium and wort agar, as well as the presence of urease activity on 8-14 days (T. soudanense it is absent) and the inability to absorb maltose and sucrose as the only sources of carbon nutrition.
M. gypseum. Soil dermatophyte causes mycoses of smooth skin and scalp. Hair is affected by the type of large-spore endotrix, the fluorescence of hair is absent or very weak.
Primary crops develop on 3-5 days. Colonies are fast-growing, flat, powdery, with age become velvety. The surface of the colonies is creamy, the reverse side has a variety of pigmentation.
Numerous lumpy, spindle-shaped, thin-walled macroconidia of 3-9 cells can be seen in microscopy. They are located on mycelium one by one or in bunches. Occasionally, there are few microconidia. The minimum inhibitory concentration of griseofulvin is from 1 to 10 µg/ml.
The fungus differs from similar cultures of M. cookei in the absence of red pigment, thin-walled macroconidia and the presence of perfect forms of Nannizzia gypsea, N. incurvata.
M. nanum. The zoophilic fungus is common in North America and Australia, causes skin and scalp mycoses. Hair is affected by the type of large-sports ectodotrix, fluorescence is absent or weak.
Первичные культуры развиваются на 6-8 день. Колонии быстрорастущие, плоские, пушистые, с возрастом мучнистые. Цвет поверхности от белого до кремового, обратная сторона красноватая.
При микроскопии отмечается обилие характерных овальных и грушевидных тонкостенных макроконидий, состоящих из 1-3 клеток. Редкие булавовидные микроконидии. Совершенная форма Nannizzia obtusa.
Trichophyton Rod.
T. mentagrophytes. Has two main varieties of mentagrophytes:
- var. gypseum (powdery);
- var. interdigitale (fluffy). The fungus causes mycoses of smooth skin, nails, less often of the scalp in humans. Hair is affected by the type of finely sporty ectotrix, does not fluorescence. The hypoid variant is distinguished from rodents and large mammals.
Primary crops develop on 5-7 days. Colonies are rapidly growing, have differences in both variants:
- In gypsum-like they are mealy, sometimes folded; the surface is creamy, the back side is brown;
- fluffy, they are flat, velvety and fluffy, somewhat powdery with age; the surface is white, the back side is yellow-brown.
In microscopy, the plaster variant has an abundance of rounded, less often pear-shaped microconidia, often arranged in bunches. In the fluffy variant, the number of microconidia is moderate. Both variants have 5-8-cell smooth and thin-walled macroconidia and have different number of curls and spirals. The minimum concentration of grizeofulvin, which suppresses the growth of the fungus, is 5 µg/ml.
Perfect forms of fungus Arthroderma benhamiae, A. van-breuseghemii.
Unlike similar T. equinum cultures, the fungus grows well on human hair in vitro and forms perforators, does not need nicotinic acid for its growth. The day of differentiation from similar cultures of T. simii it should be remembered that macroconidia of T. simii are prone to the formation of chlamydospors and decay, and that the microconidia of T. simii are polymorphic and the hair of guinea pigs are affected by it in the type of ectodotrix with green fluorescence.
Т. rubrum (synonyms of T. purpureum, E. rubrum). Anthropophile.
The predominant pathogen for onychomycosis, mycosis of the feet, hands, skin in the area of folds and smooth skin. Hair strikes rarely, without fluorescence.
Primary crops develop on 8-10 days. Colonies are fast-growing, velvety (sometimes powdery or wrinkled). The surface is white (pink or wine red at the edges), the back side is purple, red. The pigment does not diffuse in the environment. Urease does not produce. No need for vitamins.
In microscopy, numerous polymorphic microconidia, located on both sides of the hyphae, or less often in clusters, are observed. Rare macroconidia of 3-5 cells are similar in shape to a "pencil". In 95% of the strains tested, the minimum inhibitory concentration of griseofulvin is 2.5 µg/ml and below, while individual strains are inhibited by 5 and 7.5 µg/ml.
Atypical non-pigmental strains of T. rubrum can be differentiated from T. mentagrophytes var. interdigitale by the absence of perforator organs on the hair in vitro, by delayed (by 8-21) or absent urease activity and by greater sensitivity to griseofulvin. The formation of pigment by T. rubrum cultures is stimulated on Saburo environment, on potato, corn or soy agar. From similar cultures T. rubrum mushroom differs in the presence of urease activity. It can be distinguished from similar cultures of T. megninii by the lack of need for L-histidine.
T. schoenleinii (synonymous with Achorion schoenleinii).
It affects the scalp and smooth skin with the formation of sculls (favaux). Hair has weak light green fluorescence.
Colonies are slow-growing, elevated, folded with a leathery-wax surface, sometimes with a short cannon. The surface color is gray to cream, the back side is yellow. Scalloped hyphae, deer antlers, fava chandeliers can be noted in microscopy. Lots of chlamydospores. No conidia. The minimum inhibitory concentration of griseofulvin is 1-2.5 µg/ml.
T. verrucosum differs from similar cultures by the nature of hair damage and the ability to grow on media without thiamine. From cultures M. ferrugineum differs in the nature of hair damage and the ability to absorb urea as the only source of nitrogen nutrition. T. ferrugineum differs from the cultures by its clinical picture of the lesion caused and less pigmented colonies.
T. tonsurans (synonyms of T. acuminatum, T. cerebriforme, T. crateriforme, T. sulfureum). Anthropophilus.
It affects the hairy part of the scalp, smooth skin, occasionally nails, causes sycosis. Hair is affected by the endotrix type, does not fluorescence.
Cultures develop on 4-6 days. Colonies are slow growing, dry, dense, mealy, wrinkled. The surface is gray or creamy, the reverse side is from brown to ochre.
In microscopy, there is an abundance of polymorphic microconidia, rare spindle-like macroconidia. When the culture ages, there is an abundance of chlamydospor and arthrospor. The growth of cultures is stimulated by thiamine. It splits the urea. Minimal inhibitory growth concentration of griseofulvin from 1 to 10 mkg/ml.
T. equinum differs from similar cultures by the type of hair lesion and the need for thiamine. From cultures T. rubrum differs in the need for thiamine and rapid (in 8 days) hydrolysis of urea. From cultures T. soudanense differs in pigmentation of colonies, the need for thiamine, the presence of urease and absence of hemolytic activity.
Т. verrucosum (synonyms of T. album, T. ochraceum, T. discoides).
Zoophilic dermatophyte (cattle, wild and domestic animals) affects the smooth skin, less often the scalp. Hair is affected by the type of large sporadic ectotrix, does not fluorescence.
Primary crops develop from 10 to 30 days. Optimal growth temperature 37 °. Colonies slowly growing, folded, leathery-wax, sometimes velvety-powdery. The surface is gray, creamy, the back side is yellowish.
In microscopy, there are favial chandeliers, antlers of deer, numerous chlamydospores. In mealy cultures, microconidia and macroconidia, which have the characteristic form of "rat tail", are observed. Culture growth is stimulated by thiamine and vitamins (inosite). The minimum inhibitory concentration of grizeofulvin is 1-5 mkg/ml.
From similar cultures T. schoenleinii mushroom can be distinguished by its origin from the characteristic centers of lesions, the nature of the hair, the need for vitamins. From cultures T. sopsep-tricum differs in the nature of the caused clinical lesions and the need for vitamins. From the cultures of T. yaoundei differs in pigmentation of colonies and the need for vitamins.
Т. violaceum (synonyms of T. glabrum, T. puinosum).
It affects the scalp hair part, smooth skin. Hair is affected by the type of endotrix, not fluorescent.
Cultures develop on 15-20 days. Colonies are slowly growing, folded, raised, waxy, purple on the surface and back side. Non-pigmented variants are called T. glabrum.
Conidia are usually absent or very rare. In microscopy you can see scalloped hyphae, favial chandeliers, in old cultures of the chain chlamydospor or arthrospor mycelium. The growth of cultures is stimulated by thiamine. The minimum inhibitory concentration of griseofulvin is 1-10 mkg/ml.
The fungus can be distinguished from T. yaoundei cultures by its pigment and by the stimulation of growth with thiamine. From similar cultures T. gourvilii differs in the absence of microconidia, growth stimulation with thiamine and presence of urease activity.
Determination of drug sensitivity of dermatophytes
Sensitivity of dermatophytes to griseofulvin and imida-zole drugs has species differences and can change during treatment. Therefore, for rational treatment of dermatophytes, it is recommended to determine the sensitivity of the pathogens to the applied preparation in vitro.
Method of serial dilution in agar medium. The supplement (tablet, content of the ampoule) of the preparation is dissolved in water (imida ash) and in dimethylsulfatide (griseofulvin) up to the concentration of 10mg/ml (=10 000 mkg/ml). The solution is diluted 10 times with distilled water and in certain amounts is introduced into flasks with molten cooling medium Saburo to final concentration of preparations 0,1-1-2-3-4-5-10-50-100 mkg/ml. After mixing the medium is poured into Petri dishes and dried.
Suspensions of cultures are cooked on the surface of agar media by means of a bacteriological loop on a template placed under a Petri dish or by means of a multi-pin metal replicator. The crops are sown in 3 repetitions. Cups without antibiotics serve as a control. As biological control, 1-2 test strains with known drug sensitivity should be included in the experiment.
Sown cups are incubated with lids down in the thermostat at 27 ° for 7-14 days. MIC is determined by the cup with the greatest dilution of the drug, in which there is no visible culture growth.
Clinical classification of fungal diseases
The clinical picture of fungal diseases is different in originality and variety of manifestations. However, in the vast majority of cases, the introduction into the skin of mushrooms of a certain type leads to the appearance of a corresponding clinical picture. On the other hand, different properties of fungi, such as microsporia and surface trichophytosis agents may cause the same clinical manifestations.
It is generally accepted opinion that the whole variety of clinical picture of fungal diseases depends mainly on two factors - virulence of a certain type of fungi and reactivity of the patient's body, his skin.
The degree of virulence (activity), species properties, tropism of fungi play an essential role in the emergence and development of the pathological process. In addition to the properties of the causative agent, the clinical picture of fungal disease is largely determined by the nature of the body's reaction to the impact of a pathogenic fungus. Here play a role not only the anatomical localization of the process, its duration, age and individual characteristics of the carrier of the infection, but also the state of the nervous and immune systems.
In 1929, Langeroka proposed a classification of fungal diseases based on pathological and anatomical data and clinical signs of dermatomycosis. He distinguished 4 groups of mycoses: epidermomycosis, skin mycosis, trichomycosis and mycotic onychia. The disadvantage of this classification is that it is based on common morphological features, so the same disease can be attributed to different groups.
Academician O.N. Podvysotskaya in her classification of dermatomycoses (1929) divides them into the following groups depending on the location of the pathogen:
- epidermophytoses characterized by the defeat of one epithelium - multicolored lichen, erythritis, epidermophytosis;
- dermatomycoses with the localization of fungi in the dermis and hair - trichophytosis, microsporia, scabies (favus);
- deep mycoses with the spread of the process beyond the dermis.
The most common classification of Unna, supplemented by N.A. Chernogubov, divides all diseases caused by pathogenic fungi into three groups:
- epidermomycosis (branched lichen, erythrazma);
- surface dermatomycoses (favus, trichophytosis, microsports);
- deep dermatomycoses.
There are also disadvantages of this classification, because a number of mycoses (epidermophytosis, superficial yeast lesions of the skin) have not found their place in any of the groups of this classification.
Classification proposed by Professor AM. Arievich, divides all fungal skin diseases into the following major groups:
- Pilomycosis (trichophytosis, microsporia and scabies (favus).
- Epidermomycosis (epidermophytosis, rubrophytosis and superficial yeast lesions of the skin).
- Keratomycoses (colorful lichen, erythrazma).
- Deep mycosis (actinomycosis, blastomycosis, chromomycosis, sporotrichosis).
In our country, the most common is the classification of Professor N.D. Shklakov (1976). He identified four groups of mycosis and pseudomycosis:
- Keratomycoses (multicolored lichen, piedra, tiled mycose-tokelo);
- Dermatomycoses: inguinal epidermophytosis, mycosis caused by red trichophyton, trichophytosis, microsporia, fava;
- Candidosis (superficial skin and mucous membrane candidiasis, visceral candidiasis, chronic generalized, granulomatous candidiasis);
- Deep (visceral, systemic) mycoses (histoplasmosis, coccidioidosis, blastomycosis, cryptococcosis, geotrichosis, chromomycosis, rhinosporidiosis, aspergillosis, penicillinosis, mucrosis).
The group of pseudomycosis includes surface forms (erythroma, axillary trichomycosis) and deep forms (actinomycosis, micromonosporosis, nocardiosis, micetoms).
We consider the most modern and convenient classification of Professor Shklakov N.D. depending on the etiology of the causative agent, epidemiology of the disease.
Classification of dermatomycosis:
- Keratomycosis (multicolored lichen, piedra, tokelo);
- Candidioses (superficial skin and mucous membranes candidiasis, paroniasis and onychia candidiasis, chronic granulomatous candidiasis);
- Dermatophytosis:
- inguinal epidermophytiya B) mycosis of the feet
- onychomycosis
- generalized mycosis (rubromycosis)
- microsports
- surface trichophytosis
- infiltrative trichophytosis
- flavour
Mycotoxicosis and mycogenic sensitization. According to WHO classification (ICB code) mycoses of skin and mucous membranes are divided:
- Dermatophytosis
- Dermatophytes of the scalp and beard area. Microsporia of the scalp.
Favus (parsha).
Infiltrative-negative trichophytosis. Dermatophytosis of the region of the beard and mustache.
- Dermatophytosis of nails (onychomycosis). The distal form of onychomycosis. Superficial form of onychomycosis. The proximal form of onychomycosis.
- Dermatophytosis of the hands.
- Dermatophytosis of the feet. Squamous form of the Interfinger Form. Dyshydrotic form. Acute form.
- Smooth dermatophytosis of the skin: Cerebral mycosis.
Inguinal dermatophytosis.
- Malassesioses of the skin. Multicolored branched lichen. Malassesia (English) - folliculitis. Neonatal pustules.
- Candidosis of the skin and mucous membranes. Candidosis of the oral cavity.
- Vaginal candidiasis.
- Candidosis of skin.
Clinical Classification:
Keratomycoses (Malassesioses) of skin
Synonyms: Pityriasis versicolor, Yellow branched lichen Pospelov.
The disease was first described by Roben in 1853. The culture of the pathogen was first obtained by E.I. Kotlyar in 1892.
The causative agent is Pityrosporum orbiculare, which was classified by Gordon in 1951 as yeastlike fungi.
In the modern classification colorful lichen is a disease included in the classification "Malassezia - infections". Skin lesions associated with fungi of the genus Malassezia include: multicolored lichen, folliculitis, seborrheic dermatitis and some other chronic dermatoses.
Malassezia furfur, M. globose, M. Sympodialis are considered to be the causative agent of colorful lichens. Previously called pityrasporum orbiculare.
Mushrooms Malassezia live on human skin. It is believed that at least 90% of the total population are carriers of these mushrooms, causing a colorful branched lichen. This disease is widespread everywhere, affecting up to 10% of the entire population in hot countries, colored herpes are more common. In middle latitudes, most cases occur in the summer period. Adults and young people are sicker more often, the greatest morbidity is at the age of 20 years.
The development of the disease is promoted by low nutrition, increased sweating, seborrhea, reduced physiological flaking of the skin, pathology of internal organs, secretion glands. The disease is chronic, has a tendency to relapse. The disease is malocontagious, arising under favorable conditions, especially with immunodeficiency (HIV infection).
Hereditary predisposition to the disease is not excluded. As an occupational disease, colorful herpes may be more common in persons engaged in physical labor, sweating heavily.
The generic name Malassezia was first proposed in 1889, but in fact to date, for the causative agent of the multicolored lichen has survived the name proposed by Sabouraud (1904): Pityrosporum orbiculare. For microorganisms isolated from the scalp, the term Pityrosporum ovale was used. Now all these terms are combined into a single generic name Malassezia, which has 7 species, of which the main M. furfur, M. globosa. Mushrooms Malassezia - imperfect yeast mushrooms, basidomycetes. They reproduce by kidney, are polymorphic.
Multicolored branched lichen
Clinic: On the skin of the body, mainly the chest and back, a little less often on the upper limbs, genitals and face, it is extremely rare on the scalp peripheral, growing, sharply limited spots of yellowish pinkish to the color of coffee with milk and darker color. These spots vary in size and shape, but for the most part they have irregular, geographical outlines. They are characterized by extremely fine, slight peeling, which occurs as a result of the fungus loosening the surface areas of the stratum corneum, which explains the name - branched lichen.
Subjective sensations are usually absent, only sometimes patients complain of a slight itch with strong perspiration.
After ultraviolet irradiation, white pseudo-chromic spots (secondary leukoderm) remain on the affected skin areas.
The disease is characterized by years of recurrent flow.
Diagnosis: In typical cases, clinical diagnosis is not difficult. Auxiliary methods may be the following:
- Increased peeling during scraping, as a result of loosening of the stratum corneum - a symptom of chips ("nail bump") - a symptom of Benier.
- When smearing with iodine tincture (Balzer's sample), skin areas affected by the fungus are dyed more intensely than neighboring healthy areas, due to loosening of the cornea layer.
- The affected areas of the skin in the rays of a Voodoo luminescent lamp give a golden yellow or brownish glow.
- On the medium Saburo with the addition of streptomycin and penicillin (100 IU per 1 ml) or chlorotetracycline hydrochloride and olive oil at t 35-37 ° C on 7-8 day grows whitish creamy shiny yeast colony with kidney cells.
The disease is different from syphilic leukoderma, psoriasis, pink depriving Giber, erythema, vitiligo, seborrhea.
Syphilitic leukoderm is a disorder of pigmentation of the skin, which occurs in patients most often in the first few months after infection, less often later. The main clinical symptom is the appearance of combined areas of hyper and depigmentation of the skin. At sites of hyperpigmentation appear light hypopigmented spots, rounded or oval shape up to 1-2 cm in diameter. These spots are usually located at different distances from each other, they have the same size. In the foci of pigmented syphilis the surface and consistency of the skin are normal, there are no signs of inflammation, peeling and subjective disorders. Pigment syphilis is most often localized on the back and side surfaces of the neck as a necklace (Necklace of Venus). In addition, Balzer's sample will be negative, and KCS is sharply positive.
Treatment: It is mainly performed with external medicines in the form of solutions, creams, ointments. The range of fungicidal and fungistatic agents is quite wide: (lamisil, herbagen, lozeril, clochthrimasol, etc.). You can use terbisil in the form of 1% cream 2 times a day for 10-14 days. In case of frequent relapses, mycosist is prescribed 50 mg for 2-4 weeks. From traditional forms of treatment it is possible to recommend lubrication of foci with 2% iodine alcohol solution, 60% solutions of sodium thiosulphate and 6% hydrochloric acid solution by Demjanovich method, 5%-10% with sulfur-degty ointment. It is necessary to examine and treat all family members, to disinfect clothes, bedding and bed linen.
Nodular trichosporia (Piedra)
Symptoms: Bedel's disease, nodular trichomycosis, Ozori trichosporia.
Nodular trichosporia (Piedra from the Spanish Piedra stone) - Disease of the hair cuticle with the formation of white (piedra alba) or black (piedra nigra) nodules.
White (European) piedra is described by domestic dermatologists K. Lindeman, Y. Knoch in 1866, as well as foreign authors Beigell, Ozozi in 1869, "true" (black) piedra described Desenne in 1878.
The causative agent of the white piedra is Trichosporon Beigellii, while the black piedra is Trichosporon Hortai (syn. Piedraria hortae), which refers to yeastlike mushrooms.
The development of the disease is promoted by a warm climate, washing the hair with water from unstable ponds, sour milk, treatment of hair with mineral oils. The white piedra is sporadically found in Central Asia, Transcaucasia, but mainly detected in Great Britain, Hungary, Spain, France, USA and Japan.
The black piedra is spread mainly in Central and South America, Africa, India, China, Burma, Thailand.
The causative agent is the mold fungus Piedraria hortai. The life cycle of the causative agent takes place in the nodules of the black piedra on the hair. Affects mainly young people of both sexes. The disease is malocontagious, but it is possible in the endemic areas of the disease outbreak. Transmission is possible through ridges, combs.
CLINICA: The disease is characterized by a chronic course. It occurs in both sexes, but more often in women who use lactic acid products when washing their heads.
The hairs on the head, beard, moustache, as well as in the genital area are affected by white piedra.
With a black piedra, only the hair on the head is affected.
The hair is formed by multiple small, very hard nodules (up to 20-30 on each hair) irregular oval, spindle-shaped, almost completely covering the hair. Sometimes they merge to form a short (up to 1-2 mm) or long (up to 10 mm and more) clutch with a black piedre, consisting of a tightly bonded mycelium and spores of the fungus. The nodules are easily defined by palpation. Sometimes, when the hair is tightly pulled, the nodules stick together to form bundles that look like sheaves of cereals (Colombian knots). When bending such hair you can hear a kind of crunch caused by the destruction of the dense colony of mushrooms. Hair at the piedra does not break, because not only the substance, but also the cuticle of the hair is not involved in the process.
With a black piedra, the nodules are either brownish or brownish, although they may have a reddish or grayish tint.
With white piedra nodules are light, grayish yellowish or dairy mat.
DIAGNOSE is easily established based on specific clinical symptoms. In difficult cases, the diagnosis can be confirmed by a microscopic and cultural study.
In the nodules on the hair at the microscopy reveals a wide (4-6 microns) mycelium, broken down into oval, round or rectangular arthrospores, arranged in a mosaic or clusters.
On the medium of Saburo formed grayish-yellow, dark-cream, black colonies. Black piedra agents have asks with 2-8 ascospors up to 50 microns in diameter.
The piedra is differentiated from the so-called false piedra, caused by bacteria that form porous cream colonies with festoon-colored edges on the Saburo environment on the periphery.
The treatment of white and black piedra is more often only external. Patients are recommended to shave the affected area, antiseptics are used, for example, hot solution of sulfate - 1:1000-1:2000, 0.01% sulfate vinegar or 2% salicylic acid solution with subsequent combing by frequent combing of nodules. It is possible to use imdosol creams and taking inside the lamizy-la 250 mg per day for 6 weeks in the treatment of black piedra.
Tile mycosis (Tokyo)
SINONES: Tropical circular mycosis, flaky lichen, chronic figure dermatomycosis, tropical ichthyosis, herpes of Mansohn.
Tropical round mycosis is a typical epidermomycosis of tropical countries.
Tiled mycosis was first described in the Philippines in 1686 by the famous English navigator William Dempier in his book "Journey around the world. The interest in this disease was caused by the unusual kind of patients: in neglected cases, the whole skin seems to be bizarrely painted due to eccentrically located and tightly seated scales on each other. Such patients were then shown before the visiting Europeans as an attraction "man-fish" or "lizard man".
In dermatological literature, this disease was first described in 1832 by Albert.
Cerebral mycosis in tropical countries is particularly common in areas with high humidity. Epidemic foci are found in Africa (Zaire, Kenya, Sudan, Congo, Cameroon), Southern and Central Africa, in the south of India, in China, Indonesia, Vietnam, Laos, on islands of the Pacific Ocean.
A more detailed study of this disease allowed classifying the causative agent as Trichophyton concentricum, so it can be referred to dermatophytes.
Tokyo causative agent is anthropophilic dermatophyte, it does not affect hair.
The predisposing factors are poor body hygiene, high humidity and associated maceration and loosening of the epidermis. Tile-like mycosis is particularly contagious in adults. Children get sick much less often, possible ways of infection may be direct contact with the patient, as well as household items, especially bedding and bed linen.
KLINICA: Tiled mycosis is characterized by more or less pronounced itching of the skin, which is especially intense on hot days, after sweating, eating alcohol, eating salty food and even swimming in sea water.
The process is localized mainly on the torso, extensor surfaces of the extremities, buttocks and less often on other parts of the body.
Usually free from rash palms, soles and large folds. Hair and nails are not affected by the fungus.
The disease begins with the appearance of small non-inflammatory light-brown color on the body, sometimes darker or, conversely, whitish spots of rounded or oval shape, sometimes surrounded by a narrow narrow inflammatory whisk. Soon, the spots acquire a darker hue and become richly brown. As each stain grows eccentrically and grows in size, a slight and then more noticeable peeling appears in the center. In this case, the rejection of scales is incomplete; they remain tightly attached to the periphery of the rings, at the inner edge, rise as if hanging over the center. Soon, in the center of the peeling zone, as the scales fall off, begins to look at an island of clinically almost normal skin, which, increasing in size, becomes clearly visible.
Thus, in the formed skin rashes with their rounded contours, we can identify a slightly discolored central zone bordered by a corolla of overhanging scales, which in turn is surrounded by a dark brown hyperpigmentation ring.
Soon a small light brownish spot appears in the center of these elements in place of clinically almost normal skin, which in turn, as well as the original spot, performs the same development cycle. A similar path of development is characteristic of all subsequent spots, as a result, already a few months after infection, the patient's skin is covered with many rounded plaques consisting of eccentrically located gentle peeling rings. Often they are compared with the sand dunes of the coast, as from the outside of the scales quite tightly adhere to the skin, on the inside, on the contrary, slightly rise up and, freely overhanging, find one on top of the other like a roof tile or fish scales. The process can occupy large parts of the body, and sometimes only the skin and scalp are free of rashes.
When the process extends to the feet may appear hyperkeratosis and cracks that can cause pain while walking. Hair is never involved in the pathological process.
The disease is very persistent, has a chronic nature and can last for a long time, and in the absence of treatment - even decades. On the part of the general state of the body there are usually no deviations.
Diagnosis of tiled mycosis Tokyo is simple and based on typical clinical symptomatology. In dubious cases, microscopy in scales can detect a dense network of branching yarns of fungus mycelium with spores. In case of cultural diagnostics (Trichophyton concentricum culture grows slowly), fungus colonies grow, which look a little like Trichophyton faviforme.
Treatment and prophylaxis
Warm baths with subsequent treatment of affected pumice stone hearths and application of various keratolytic ointments, especially with salicylic acid, sulfur are shown daily. In common processes it is possible to carry out treatment by Demjanovich method (60% solution of sodium thiosulphate and 6% solution of hydrochloric acid), the use of lamisyl sprays is shown. In the generalized process of taking inside terbisil (1 tablet once a day for 2 weeks) Prophylactic measures are reduced primarily to the observance of body hygiene and the fight against hyperhidrosis. The disease is chronic, persistent and prone to recurrence.
Candidosis
Synonyms: Candidamycosis, coormicosis, superficial blastomycosis.
Fungal disease of the skin, mucous membranes and internal organs caused by the fungi of the genus candida. The disease was known to doctors in ancient times (stomata aphtoides, aphta infantis). It was first described by B. Langenbeck in 1839, mushrooms in tissues were found in 1843 by Berg, and in 1923 Berkhout identified the genus Candida among yeastlike organisms. The disease is found in all countries of the world, but is most common in the tropics and subtropics.
Etiology
Pathogens: Candida albicans, less often other species - Candida tropicalis, Candida pseudotropicalis and others. More than 100 species of fungi have been described in the genus Candida.
Fungi of this genus are attributed to conditionally pathogenic microorganisms; as saprophytes they are widely distributed in nature, are found on the skin, mucous membranes and in the feces of almost a fifth of healthy people. Fungi of this genus are associated with normal microflora of the skin (up to 20%) and intestines (up to 0.5%) in humans. The source of infection may be a person suffering from candidiasis (kissing, sexual intercourse, dishes, infection of newborns through infected birth routes). Infection is promoted by humid climate, maceration of the epidermis, manual treatment of vegetables, fruits, berries in tinned and confectionery production, violations of hygiene rules in the nursery. The endogenous path of infection is associated with the activation of candidiasis flora available in the body in microbial associations (the development of secondary candidiasis in pneumonia, tuberculosis, neoplasm, etc.).
Among the pathogenetic factors include immunodeficiency, endocrinopathy, hypovitaminosis, metabolic disorders, chronic diseases, the use of broad-spectrum antibiotics, cytostatics, radiation exposure and other means of reducing the natural resistance of the body.
The genus Candida (Candida) includes unspoiled yeast, in which pseudomycelium may be well developed, rudimentary or absent. Some species form true mycelium. The mushrooms of the genus Candida do not form carotenoid pigments, which distinguishes them from Rhodotorula, and do not form capsules, typical for cryptococci. In addition to chlamydospor, which is a sign of one species (C.albicans), these mushrooms do not form other types of spores - asco-, ballist-, telio- or arthrospor.
The yeast phase of Candida is represented by single-celled organisms of relatively large size - 1.5-8x1.5-14 microns, oval, rounded or elongated shape. They grow relatively rapidly on dense and liquid nutrients, better with the addition of carbohydrates.
Optimal growth temperature 25-28 ° C; pathogenic to humans and animals species grow at 37 ° C, marginal temperature points - 5-40 ° C. Optimum pH - 5.8-6.5, but fungi can grow at more acidic reaction of the medium (pH 2.5-3.0). Reproduction of fungi is carried out by multipolar kidney, by biochemical properties they are optional anaerobes.
Cell wall of fungi consists of 5-7 layers.
In case of tissue infestation, yeast cells are partially transformed into a micelial (nitchy) phase. Mycelium cell wall consists of 3 layers and is largely inferior in thickness to the similar structure of the yeast phase. The mycelial form of the fungus has a common cell wall and transverse partitions, which allows this structure to be attributed to a true mycelium. Typical for both growth phases is the predominance of transparent layers in the cell wall composition over electron-dense layers.
Pseudomycelium is formed as a result of incomplete budding: the formed daughter cell keeps the connection with the mother through a narrow isthmus of the outer layers of the cell wall.
Only some species of Candida have etiological significance for humans and animals.
Characteristics of some Candida species:
- C. albicans on a dense medium forms convex colonies of white or cream color sour creamy consistency: yeast cells of oval or elongate-oval shape with the size of 2.9-7.2x2.9-14.4 microns, filamentize irregularly, clusters of yeast cells (glomeruli) strongly refract light and have almost black color. The predominant spherical type of growth, and glomeruli due to close adhesion to each other in the growth process deform its original spherical shape. At the periphery of the threads there is a type of Candida, and can be identified and wing type. In the process of exhaustion in the glucose environment (in 4-7 days) or on special media (rice agar) on the terminal threads of pseudomycelia are formed chlamydospora - two-contour formations with granular content. At the place of attachment of chlamydospora sometimes thickening is formed - protochlamydospora. The diameter of chlamydospors is almost 2 times greater than the cross section of the carrier cell. For epidanalysis purposes, a typical C.albicans identification may be of interest. The phenotypic differences are reduced to the following features: C. stellatoidea is completely identical to C.albicans (filamentation, chlamydospores, RB-effect), differing only in the absence of sucrose and galactose assimilation; C. claussenii filamentis according to the type of Micocandide and does not give RB-effect; C. claussenii does not form chlamydospores. C.albicans dominates sharply among different types of Candida, which are detected in both patients and mykonositors.
- C. albicans form creamy, white or gray colonies, smooth or folded. Yeast cells are ovoid-shaped, 4.3-7.2x5.8-10.8 microns in size. Pseudomycelium is abundant, consisting of long branched yarns. The predominant growth type is Mycotoruloides, there is a Candida type and rarely a spherical one.
- C. krusei. Colonies are flat, white or matt, voile-like, with uneven edges, soft consistency. A soft film and a high parietal ring are formed on the liquid medium. Yeast cells are oval, elongated or cylindrical in size 2.2-5.6x4.3-15.2 microns, arranged individually or as a chain. Bountiful pseudomycelium is formed quickly and uniformly along the dashboard. The growth type Mycocandida prevails, but the types Mycotoruloides and Candida occur.
- C. kefyr (C.pseudotropicalis). Colonies from creamy to yellowish, soft consistency, smooth or finely mesh surface. Ovoid-shaped yeast cells 2.5-9x5-15 microns in size. The intensity of filamentation varies in different strains, the predominant growth type is Mikocandida.
- C. pa rapsilosis. Colonies ranging from creamy to yellow colored, are soft, most strains are smooth, some are partially or completely folded. Yeast cells are oval, ellipsoidal or elongated, sizes 2.9-4.3x3.6-7.2 microns. The predominant growth type of Mikocandidate. C.parapsilosis is a frequent pathogen of onychomycosis.
- C. guilliermondiu Colony yellow cream color, with smooth shiny surface, soft consistency. There are variants with a matte surface and exhaustion. Yeast cells are relatively small (2-4,5x2,5-7 microns), more often ovoid, less often cylindrical in shape. The degree of pseudomycelium development varies in different strains. In terminal sites Candida type prevails, glomeruli formed in the course of threads have a spherical shape, sometimes resembling a bunch of grapes. Because of weak refraction of light in structure of glomeruli small yeast cells of the round form are well visible.
- C. utitts. Colonies with smooth surface, soft consistency, color varies from grayish to creamy. Yeast cells from ovoid to cylindrical shape, their size is 3.5-4.5x7-13 microns. It forms a primitive pseudomycelium consisting of rough short branches carrying rare ovoid cells.
- C. catenulata (C. brumptii). Colonies of soft consistency with folded surface, dull color - from grayish to creamy. Yeast cells are ovoid or elongated, often pear-shaped or curved ("sausage" shape). Cell sizes are 1.5-5.5x2.9-8.8 microns. Growth type - Candida. Pseudomycelium consists of branched filaments of short pseudo dykes or long ovoid cells. Pseudogyphs are often curved or wave-shaped, often with swollen cross sections.
All Candida species assimilate glucose as a source of carbon and ammonium sulphide as a source of nitrogen.
According to the antigenic structure, Candida is a heterogeneous group with both related and isolated species inside.
C. albicans strains have 2 serotypes - A and B. Close in their antigenic structure to C. tropicalis. The strains of C. albicans which are close in their antigenic structure to C. atellatoidea are referred to serotype B.
Epidemiology of pathogens
Carriers of C.albicans are more than 20 species of animals, but cases of candidiasis in animals are extremely rare. It is interesting that in the external environment (grass, water, soil, bedding for livestock, air in the enclosure) C.albicans were detected only during the outbreak of candidiasis; attempts to detect these fungi in the extra-zepidemic period were unsuccessful.
Other species of Candida fungi are found quite often in the external environment. C. catenulata (C. brumptii), C. parapsilosis, C. curvata, C. humicola and C. tropicalis are widely represented in soil; C. kefyr (C. macedoniensis), C. lipolytica and C. scotii are less frequently distinguished. C. guilliermondii, C. ragardiis, C. kefyr (C. pseudotropkalis), C. tropicalis and C. lipolytica were isolated from the air. 26 strains of C. krusei were isolated from 30 samples of sour wine berries In a study of 26 foodstuffs it was found that the most abundant fungi of the genus Candida were cottage cheese, curds, ice cream and sour cream. Prostostokvash, acidophiline and cream products either did not contain Candida, or these mushrooms were present in minimal quantities. The species composition was dominated by C. krusei (55.4%) and C. kefyr (C. pseudotropicalis) - 31.4%, as well as C. albicans and C. tropicalis (7.1% and 6.1% respectively).
Generalized data on the breadth of Candida fungi in the external environment and on food products were presented by J. Kefyr (C. pseudotropicalis). Coudert (1955):
- C. guilliermondii - flowers, tobacco, confitures;
- C. lipofytica - margarine, olives;
- C. macedoniensis - commercial yeast;
- C. mycoderma (C.vini) - dry wines, beer;
- C. pulcherrima - flowers, fruits, honey;
- C. tropicalis - rotting plants, dry tea leaves;
- C. zeylanoides - frozen beef.
In humans, the frequency of carrying fungi of the genus Candida reveals a tendency to increase: if in the 20's it was 10% on the mucous membrane of the mouth cavity, in the 60-70's it rose to 46-52%.
On the vaginal mucosa of non-pregnant women, the carrier reaches 11-12.7%, but it increases dramatically in the last third of pregnancy, and according to various data, it ranges from 30% to 86%. In faeces the frequency of detection of Candida reaches 80%, on intact skin - up to 9.5%. The frequency of Candida vulvovaginitis in pregnant women is 10-20 times higher than in the control group. It is assumed that pregnancy is a predisposing factor for the development of candidiasis due to the immunosuppressive effect of high levels of progesterone and the presence in the serum of immunosuppressor factor associated with alpha globulin.
Rapid and intense colonization of a newborn child's body leads to the formation of hypersensitivity of the delayed type (DHT) to C.albicans antigens in 60% of children by the end of the first year of life.
Pathogenesis
In the pathogenesis of candidiasis there is a distinction between exogenous and endogenous favorable factors.
Exogenous factors include: injuries of the skin and mucous membranes (e.g., yeast lesions of the nipples of breastfeeding mothers, damaged by children while sucking, yeast stomatitis and snacking with unsuccessful dentures, candida onychia and paronichia in injuries during manicure, etc.). ), high humidity, which leads to the spread of candidiasis in geographical latitudes characterized by a humid and warm climate, the effect on the skin of acids and alkalis that contribute to skin maceration, pathogenicity and virulence of the fungus itself. Exogenous factors influence the occurrence of candidiasis in a certain state of the macroorganism, its susceptibility to yeast fungi.
Endogenous factors that contribute to the weakening of the body's defenses and thus to the development of candidiasis are: decrease in the activity of serum fungistase, which depresses the vital activity of the yeast flora, hypovitaminosis (especially deficiency of riboflavin - vitamin Bg), metabolic diseases (diabetes, obesity), Vegetoneurosis signs (increased sweating, poor circulation of the extremities), gastrointestinal disorders, contributing to dysbacteriosis, endocrinopathy, leading to obesity, hypo- and hyperthyroidism, Itsenko-Kushing syndrome.
The use of antibiotics, especially broad-spectrum antibiotics contributes to the occurrence of intestinal dysbacteriosis, which may cause severe systemic candidiasis. To the same results may lead to the use of contraceptives (inside), corticosteroid hormones, cytostatic drugs (immunosuppressants), which cause hormonal shifts and decrease the body's resistance).
Primary infection with Candida fungi may occur in newborns during the passage of the birth tracts, which is facilitated by the increased frequency of carriage on the vaginal mucous membranes of the mother during pregnancy.
Adhesion of the fungus to epithelial cells is the first stage of its interaction with the macroorganism. The predominance of C.albicans on the mucous membranes is associated with active adhesion of yeast cells of this species to the epithelium of the oropharynx and vagina, which is most pronounced at 37 ° C and pH 7.3. However, a fairly high degree of adhesion is also observed at slightly acidic values of the medium (pH 6.0).
C. tropicalis has moderate adhesiveness, C. krusei and C. kefyr have weak adhesiveness; they are almost without adhesiveness. The degree of adhesion varies in individuals (3-4 times), as well as in the same subject when taking the epithelium on different days.
The exact mechanisms of adhesion are not clear; it was found that yeast cells in the stationary phase adhere more intensively than in the logarithmic growth stage. It was shown that different species of Candida were able to adhere to the fibrin-platelet matrix; at the same time, C.albicans possessed a high adhesiveness; the other species were arranged as follows in order of adhesive activity decrease: C. tropicaiis, C. parapsilosis, C. pseudotropicalis, C. guillier-mondii, C. krusei.
C. albicans and C. tropicaiis are capable of adhesion and penetration of vessel endothelium, to a lesser extent these properties are inherent in C. krusei and to a lesser extent in C. parapsilosis and C. pseudotropicalis. To a certain extent, these activities can explain the leading role of C. albicans and C. tropicaiis in hematogenic dislocation.
In newborn children, candidiasis is a primary infection, which is associated with the imperfection of the body's protective systems: the absence of secretory Ig A, a decrease in the levels of individual components of the complement and its overall hemolytic activity, iron saturation of the transferrin, a sharp depression of neutrophil chemotaxis (up to 2 years) and monocytes (up to 5 years), and a decreased ability to form delayed hypersensitivity (SHT).
For a long time, it was believed that the transplacental pathway of infection in candidiasis was not present, but in recent years, information on dozens of cases of congenital candidiasis has been summarized.
The prognosis of the disease in a newborn depends on the period of pregnancy: at the birth of a child after 36 weeks in the overwhelming number of cases of candidiasis has a superficial character and is easily bought; at birth in earlier terms the disease has a systemic (generalized) course and is characterized by high lethality.
It was found that a significant proportion of women who developed fetal candidiasis used intrauterine devices for a long time.
The role of irrational antibacterial therapy in the development of candidiasis is justified by a large number of studies, in which the suppression of normal microflora of the body is given crucial importance.
The development of candidiasis in the interfinger folds of the hands is facilitated by frequent contact with water, as skin maceration develops, which is a favorable environment for the introduction of the pathogen from the external environment.
A number of antibiotics have a direct stimulating effect on Candida cells, intensifying their division: some drugs are a source of nitrous substances for these fungi. Antibiotics have a suppressor effect on the immune system of the body," tetracyclines cause desquamation of the intestinal epithelium, providing the pathogen easier to penetrate into tissues.
Corticosteroids reduce the resistance of the macroorganism and contribute to the development of surface candidiasis, which may then become disseminated.
Endocrinopathies are important in the development of candidiasis: diabetes mellitus, hypoparathyroidism, a combination of hypoadrenic corticism and hypoparathyroidism, which have been combined into a single syndrome with surface candidiasis. This disease, which is transmitted by hereditary way, develops only in adolescence. Signs of candidiasis appeared in such patients on average 3.5 years after the development of endocrinopathy; accidental removal of parathyroid glands in adult strumectomy did not lead to candidiasis. The use of hormones alone did not stop the candidiasis process: antifungal antibiotics (amphotericin B) were needed to achieve a therapeutic effect.
Systematic (up to one year) use of hormonal contraceptives (noretinodrel, mestranol) causes the development of hormonal dysfunctions, which in turn leads to an increase in the frequency of Candida fungi, as well as can-didose vaginitis. It is believed that the pathogenetic role is played by the estrogen component of the contraceptive, which leads to an increase in the concentration of glucose in the blood and secretions.
Candidosis also occurs after the use of metronidazole. The development of candidiasis is associated with a direct irritant effect of the drug on mucous membranes and disturbance of local normal microflora.
Microtraumas, maceration and chemical damage to the skin contribute to the introduction of Candida fungi into tissues. Superficial and then generalized candidiasis is observed in patients with hemoblastoses accompanied by neutropenia.
Progress in the treatment of hemoblastoses has led to an increase in the life expectancy of these patients and, at the same time, an increase in the number of infections caused by opportunistic pathogens, including fungi of the genus Candida. According to the National Cancer Institute (USA), in 1954-1958 systemic candidiasis was detected in 7% of patients with acute leukemia, and in 1959-1964 in 7% of patients with acute leukemia. - у 20 %. LGentry et al. (1978) found disseminated forms of candidiasis in 76% of patients with leukemia, 26% of patients with lymphomas and 20% of patients with myeloma. One in five (21%) of acute leukemia patients was fatal due to mycotic infections with predominant candidiasis and aspergillosis.
There is no doubt about the role of T-lymphocytes (T-cells) in providing resistance to Candida in chronic skin-mucosal candidiasis. Thymus gland underdevelopment, thymic alimphaplasia in combination with agammal bulinemia, thymoma and Hodgkin's disease are background conditions for this disease.
One of the ways the pathogen enters the body and the associated systemic candidiasis is realized through parenteral interventions. Perfusion of drugs, as well as parenteral nutrition lead to local tissue irritation and ingress of candidiasis pathogens from the outside of the patient and the environment. Sounding of heart cavities, prosthetics of valves, the use of extracorporeal circulation devices, surgical interventions in the gastrointestinal tract - these are the main factors in the parenteral introduction of fungi of the genus Candida in the body. According to numerous data from foreign researchers, generalized forms of candidiasis due to hematogenic distribution of fungi are often observed in addicts, who usually completely ignore the rules of aseptics and antiseptics.
In parenteral penetration, it is not lymphocytes, but phagocytes, primarily granulocytes and monocytes, that play a crucial role in protecting the macroorganism from candidiasis. Mechanisms for protecting the macroorganism in candidiasis are detailed in the next section.
In the last decade and a half, various clinical forms of candidiasis have been registered with very high frequency in people infected with human immunodeficiency virus (i.e. HIV infection), and especially in patients with clinically developed AIDS. This was the reason for including candidiasis among the so-called "AIDS marker" diseases.
Mechanisms of macroorganism protection in candidiasis
The initial stage of colonization of the mucous membranes of the Candida fungi is their adhesion to epithelial cells, which is provided by mannan and trypsin-sensitive protein of the fungus.
Adhesias prevent the secretions of mucous membranes that contribute to the mechanical removal of fungi, as well as peroxidases and secretory immunoglobulins of class A (slgA). According to most researchers, the most important factor limiting the adhesion of fungi is normal microflora (anaerobic and aerobic microorganisms), representatives of which exhibit antagonism to Candida fungi and compete for epithelial receptors.
After the attachment of the fungus cells to the epithelium in the normal function of the immune and endocrine systems, the myconosis is formed without the development of pathological process. The equilibrium between micro- and macroorganism is provided by T-effectors of delayed hypersensitivity type (LHT), which during antigenic stimulation secrete a number of mediators, which accumulate macrophages (factor of inhibition of macrophage migration, factors of positive chemotaxis of macrophages and monocytes) and enhance their microbial activity (increase of H2O2, OH and fatty acids production).
Having overcome the epithelial barrier, yeast cells are transformed into a thread phase, forming a false or true mycelium. Mannan of the cell wall of both phases of the fungus activates the complement system through an alternative pathway, and in the presence of complement-binding antibodies simultaneously starts and the classic pathway to activate complement.
It was found that in an autonomous form, the complement system is not able to lick cells and fungi neither when activated by an alternative route, nor in the presence of complement-binding antibodies.
When fungi penetrate into body tissues, neutrophils play a crucial role in the development of inflammation. Inside neutrophils 50-58 % of C. albicans cells perish, in monocytes - about 50 %; for other types of fungi of genus Candida the percentage of cell death in neutrophils is even higher: C. krusei - 76 %, C. tropicalis - 84 %, C. pseudotropicalis - 98,5 %.
Interleukin-1 increased the candidacidity of human neutrophils; it reached its maximum after incubation within 4-6 hours.
In hematogenic distribution of C.albicans favorable conditions for their long-term preservation and reproduction are created in renal tubules, where fungi are protected from neutrophil phagocytosis. The mycelium formed penetrates into the interstitial tissue and causes the fungus elements to enter the blood. The inflammation outcome is determined by the functional state of neutrophils and their quantity. The disease prognosis worsens with a deficit of IGOs, but an extremely unfavorable outcome is observed with a deficit of HADP-oxidase and cytochrome B, which occurs in chronic granulomatous disease due to the complete absence of oxygen-dependent killing mechanism. Violation of the locomotive function of neutrophils and monocytes is extremely rare.
As for mononuclear phagocytes, they play an insignificant role in the protection of the macroorganism at the generalized can-didosis, in which the main protective function is provided by granulocytes. In chronic skin-slimy and granulomatous candidiasis, which in most patients is combined with selective immunodeficiency to fungus antigens (absence of a specific clone T-effectant GZT or its suppression), in the case of normal content of granulocytes there is no hematogenic proliferation of fungi. This once again emphasizes the role of these phagocytes in protecting the macroorganism from candidiasis infection.
Clinic
Classification. Clinical forms of candidiasis are divided into superficial (skin, mucous membranes, onychia and paronichia) and systemic, or visceral. In addition, chronic generalized (granulomatous) candidiasis of children is distinguished, which some authors consider to be an intermediate disease between superficial and visceral forms of candidiasis, and candidates (levurids) - secondary allergic rashes.
Candidosis is superficial. Candidosis of the skin. On smooth skin, small folds on the hands and feet are more often affected, less often large (inguinal and hip, armpit, under the mammary glands, buttocks).
Candidosis of large folds, or intrigenous candidiasis, or yeast опрелость. Affected inguinal and hip, buttock folds (often in infants), armpit hollows, the area under the mammary glands in women and abdominal folds in obese faces. These places have large eroded lesions of dark red color, with sharp borders and moderate humidity. On the periphery of the hearths there is a border of whitish peeling macerated epidermis. The presence around the main hearth of small hearths of the same nature is quite typical; they are called "daughter", or dropouts.
Interfinger yeast erosions in the brush area are very common. More often, women working in confectionery, canning and fruit and vegetable production, saleswomen of carbonated water, laundries, housewives are sick. Most often affected are the folds between III and IV fingers and the side surfaces of these fingers, where the horn layer is macerated, slightly swollen, has a pearlescent color or is rejected, exposing eroded, wet and shiny red surface. On the erosion boundaries, you can see fragments of macerated epidermis with a pearlescent shade. These erosions are characterized by a persistent current and a tendency to relapse, burning and itching are subjectively observed. On the feet, yeast erosions are less frequent, but occupy a greater number of interfinger folds (sometimes all the folds are affected).
Among other yeast lesions of smooth skin, which are much rarer than candidiasis of large and interfinger folds, it should be noted the yeast lesions of small folds (behind the auricles, in the area of the navel, anus, foreskin), different from lesions of large folds only in size.
Candida dermatitis in the palms and soles is characterized by hyperkeratosis, underlined pattern of skin furrows, dirty brown skin color.
Candidal dermatitis in infants and adults may be limited and widespread, erythematosquamosis or dyshydrotic. Whitish macerated epidermis on the periphery and the presence of yeast lesions in other areas of the skin make it possible to suspect the true nature of the disease.
Candidotic balanopostitis more often occurs in patients with diabetes, or as a result of infection from women with yeast vulvovaginitis. It is characterized by the appearance of the inner leaf of foreskin and the head of the penis, limited foci of hyperemia, erosion, whitish epidermis, severe itching.
The diagnosis of skin candidiasis in most cases is not difficult', is based on the originality of the clinical symptoms described above and is confirmed by laboratory diagnosis. Candidosis of large folds is differentiated from epidermophytheria of large folds, in which there are no eliminations, and with microbial eczema, which is accompanied by more or less pronounced pyogenic symptoms. In normal oprelography, the boundaries of the lesion are less sharp, there is no peeling bezel of the epidermis at the periphery and there are no sifts. In seborrheic eczema, children in folds are also marked by maceration; however, wetness is more pronounced than in candidiasis of large folds, and there is also pronounced swelling and bright hyperemia of the foci. Psoriasis of folds is characterized by significant infiltration and papuletic elements at the periphery. From Ritter's exfoliating dermatitis intertriginous candidiasis is distinguished by the absence of serous blisters, satisfactory general condition, the absence of dyspeptic and gastrointestinal disorders, as a rule. In addition, exfoliating dermatitis begins with the appearance of red spots around the mouth, spreading throughout the skin, against which there are bubbles and bubbles with gray content. In Reiter's desquamative erythrodermy, the disease begins with red edematous spots in the area of the buttocks, buttocks and inguinal folds, and then merging with each other and spreading to the abdominal and back area. The process is generalized and evenly affects the smooth skin and folds, which is rarely the case with candidiasis. In addition, the development of erythrodermia is more frequent at the age of 4-6 weeks, accompanied by severe gastrointestinal disorders, anemia and fever. In syphilic-like papule-like impetigo the main element is papules, maceration and loose porridge-like accumulations in the folds are absent.
Candidosis of mucous membranes
Yeast fungi can affect any mucous membrane (mouth cavity, conjunctivae, vulva, urethra, bladder, etc.).
Candidosis of oral mucous membranes (thrush, Soor) occurs mainly in newborns and in the first weeks of life. Adults are sick less often. At the beginning of the process on the mucous membrane of the cheeks, tongue, gums, soft sky, dotty deposits of white appear, reminiscent of mana cereal grains, which are on a hypermised background 'mucous membrane. The plaque merges and forms a solid film, which is easy to remove first, but then thickens, gets a dirty color and fits more tightly to the mucous membrane. The lesion of the mucous membrane of the tongue may be one of the manifestations of yeast stomatitis, but sometimes runs as a separate disease (yeast glossitis). In these cases, on the back of the tongue, you can see the usual strikes of the thrush or deep furrows going in different directions ("scrotal tongue"), at the bottom and along the edges of which you can see whitish patches. When whitish caps appear, resembling follicular angina, they speak of mycotic (yeast) angina, in which there is no pain during swallowing, no visible inflammatory reaction, and no fever reaction.
Candidosis of the corners of the mouth (mycotic jamming) and Candidosis Heilitis may accompany each other or be observed in isolation. Usually they occur against a background of lack of vitamin B. An underestimated bite may play a role in the pathogenesis of seizing. On a hyper-removed background occur more often bilateral macerated areas with grayish-white crumbs or films, after removal of which are visible cracks (in the corners of the mouth) or spot erosion. The red edging of the lips is slightly thickened, dry.
Candaceous vulvovaginitis
In recent years, the number of diseases of the genitourinary tract caused by yeastlike fungi of the genus Candida has increased significantly, especially in women. Candida is the second most common vaginal infection in the United States. In 1975-1984, there was an increase in the detection rate of Candida vulvaginitis (KB) in England. Up to 85% of women of reproductive age had KB at least once (one in two had KB again), and 5% of women have chronic relapsing forms of KB.
The existence of healthy carrying of Candida fungi has been proved in 13-30% of women, which is facilitated by both general reasons for colonization of macroorganism by fungi (therapy with broad-spectrum antibiotics and treatment with corticosteroid hormones) and factors specific to women (pregnancy, use of hormonal contraceptives, etc.).
The increased frequency of carrying Candida fungi on the mucous membranes of the genitals and the number of KB diseases during pregnancy may be due to an increase in the concentration of glucose and reproductive hormones in the vaginal secretion, as these hormones are a source of carbon for the fungi. The effect of such exposure is to increase the reproduction of fungal cells and stimulate the formation of micelial (invasive) phase.
In 85-90 % of patients KB is caused by the species C. albicans; among other species the etiological factor of KB is more often C. tropicalis and C. krusei.
The first stages of colonization by fungi of the vagina mucous membrane are related to the adhesion of fungal cells to epithelium. It is possible that the essential etiological significance of C. albicans may be explained by the high adhesive capacity of this species.
Epithelium avidity to Candida fungi is enhanced by estrogens, which increases the adhesive capacity of the fungus cells. In addition, the stimulating effect of estrogens directly on the adhesive activity of C. albicans has been experimentally shown. Hypeestrogenia, increased levels of reproductive hormones during pregnancy, suppression of normal vaginal flora (lactobacteria) lead to changes in the quantitative ratios of biocoenosis, creating favorable conditions for the development of the pathological process. The main function of maintaining the qualitative ratios of microbial associations of the vagina is performed by the obligate flora, represented by lactobacteria.
Chronic relapsing KB in a significant number of cases is due to endogenous strains of C. albicans, which have the same properties as the strains that survive on the mucous membranes of the vagina, vulva and intestines. The etiological role of exogenous strains, which can be carried by sexual partners, is not excluded. It has been established that chronic relapsing KB may occur against the background of immune cellular disorders and in a state of immediate hypersensitivity, although the mechanisms of such exposure are still unclear.
Clinical manifestations of KB are not specific. The most typical symptom is acute itching. Vaginal discharge is a sign that is not constant in KB; often it is minimal. In typical cases, the secretions have a curdy appearance; their consistency may vary from watery to viscous. Typical signs of KB are pain, itching, burning in the vulva and dysuria areas. The smell is not always detected and is not stinky.
During external examination, erythema and edema of the labia and vaginal mucosa are often detected; pustule and papule lesions are often detected. The cervical canal is usually unchanged. The erythema of the vaginal mucous membrane is combined with the presence of viscous whitish excretions. The characteristic feature is an exacerbation of symptoms a week before your period and some relief after the start of menstruation. Due to the impossibility to identify the etiology of the disease from the clinical picture, laboratory methods of CB diagnosis become particularly important.
As a screening method to diagnose candidiasis vulvovaginitis, it has been proposed to use the latex agglutination reaction (RAL), which uses a suspension of latex particles sensitized with antibodies to the mannanes of cell wall C. albiccms. The sensitivity of this method is 81% and the specificity of RAL reaches 98.5%.
The differential diagnosis of mucous membrane candidiasis is based on the clinical picture of lesions (presence of whitish or grayish plaque) and microscopic examination data. The thrush may resemble leukoplakia, red flattened lichen, syphilitic oral papules, aphthae and aphthous stomatitis. The first two diseases are extremely rare in children. In addition, with red flattened lichen, some elements are usually found on other parts of the skin and mucous membranes, there are no easily removable plaques or films. In syphilitic papules, there is a distinct inflammatory corolla around the papules, sharp borders and other symptoms of syphilis. Aphthae is characterized by painfulness and increased submandibular lymph nodes. Aphthous stomatitis produces multiple minor erosions with a bright inflammatory rim on the periphery, a saucer-shaped bottom covered with yellowish plaque.
Mycotic seizure has to be differentiated from streptococcal seizure, which occurs mainly in children, more often unilateral (mycotic seizure occurs mainly in adults, more often bilateral). Maceration phenomena are more typical of yeast infection, and exudation with streptococcal imethysification.
Lesions of the mucous membranes of non-yield etiology ("geographic" tongue, rhomboid glossitis, vulvovaginitis) are characterized by the absence of macerated mucous membrane areas, whitish or grayish films and curdy crumb layers.
Candidosis of nail rollers and nails
Of all yeast lesions, localization of the process in the area of nail rolls (gyronichia) and nails (onychia) is most common, mainly in women. Yeast laroniasis and onychia are often combined with interfinger erosion. The process begins with the nail roll, which becomes hyperemic, swollen, a small drop of pus can be squeezed out from under it, and the nail skin (eponychium) disappears. Then, the side parts of the roller are involved in the process. In the acute stage, there is a sharp painfulness. Usually, after the subsidence of inflammatory phenomena, the process captures the nail plate, which in the area of the hole and the side edges changes color, it turns brownish-gray. The nail plate is thinning and crumbling. It is characterized by its transverse and striped exhaustion, sometimes the nail plate is easily peeled off. Usually only the nails of the hands are affected, most often III and IV fingers.
Differential diagnosis. From onychomycosis of another etiology, the candidiasis process differs in the combination of paronichia and onychia and positive results of laboratory tests.
Candidamycides are secondary allergic rashes that occur during candidiasis. They are also called levurids (from French Levures - yeast). They occur in the hypergic state of the body, caused by the processes of sensitization. Levurids are characterized by a sudden acute appearance of erythema-tosis-scomatoid foci with their rapid dispersion and frequent presence of common phenomena, which distinguishes exemo-like mikides from true yeast lesions of eczematous nature. In addition, in the latter cases, yeast and yeast-like fungi that are absent in levurids are detected in a microscopic examination, and skin samples with the corresponding antigens produce sharply positive results. In rational therapy, levurids quickly disappear. However, in cases of irrational treatment, they may exist for a long time and even transform into eczema.
Levurids are most often formed by acute common candidiasis of mucous membranes, large folds and smooth skin. Outside the erythematosan-scomosis foci, levurids are less often of a utilitarian or bullous nature.
Chronic generalized (granulomatous) candidiasis
Generalized candidiasis is characterized by an extreme variety of clinical manifestations and absence of pathognomonic symptoms.
It is a special kind of candidiasis, detailed study of which began in the late 50-60s. In most of the cases described, the disease began in early childhood with thrush. Later, due to the use of antibiotics (usually a combination of antibiotics) for various infectious or cold-related diseases, there was a generalization of the process. In the oral cavity yeast lesions capture the mucous membrane of the cheeks, hard and soft sky and gums. Stubbornly flowing jams are formed. Macrohelium develops due to the formation of yeast heilitis. In most cases, there is a scrotal (rough) language.
Damage to the mucous membranes of the oral cavity may also begin with the appearance of limited whitish spots, sometimes merging, which are difficult to separate from the mucous membrane surface. Such lesions are often combined with the diffuse erythema of the entire mucous membrane, whose surface is dry.
Pure erythematous form, without a pronounced reaction of cervical lymph nodes and the so-called "black hairy tongue" is less frequently encountered. The latter type of lesion is characterized by hypertrophy of the papilla epithelium and an abundance of mycelial threads covering their surface. According to some data, the contact of a newborn child with the causative agent almost always leads to the development of candidiasis of varying degrees of severity. In most cases, candidiasis of the oral mucous membranes disappears spontaneously during the neonatal period.
The common process with an abundance of plaque on the oral mucous membranes in newborn babies often makes feeding difficult. Infection may spread to other parts of the gastrointestinal tract. Involvement of the esophagus leads to the child's refusal to suck, regurgitate and vomit, and later to the development of cachexia. Radiologically, in such lesions there is a narrowing of the esophagus lumen, blurring of its borders, weakening of peristalsis up to its complete absence. Ezophagoscopy usually reveals ulcerated epithelium, often drain centers of lesions, covered with white plaque, which consists of mycelium of the fungus. The degree and frequency of damage to the mucous membranes of the mouth and esophagus are not always correlated.
The lesions of the face skin (more often on the nose, cheeks, and center of the forehead), the scalp, the torso and the extremities are characterized by the appearance of hyperemic, infiltrated and peeling spots, which gradually turn into granulomatous pockets with festoon shapes. On the surface of most of the elements there are crusts, on removal of which reveals vegetation, hyperkeratosis. In all sick children, the nail rolls are infiltrated, swollen, and the nail plates are significantly thickened, deformed, have a dirty gray color. The nail skin is preserved (as opposed to yeast paronias in adults).
After the elements are resolved, scar atrophy remains on the smooth skin, and persistent baldness develops on the scalp in place of the centers.
Most of these children have recurrent pneumonia, bronchitis, diarrhea, and in X-ray examination - amplification of the bronchosovascular pattern, compaction of lung tissue in the root areas, etc. Periodically, there are sudden increases in body temperature to 38-39 ° C with a rapid fall.
Stomach damage is accompanied by the development of blunt pain in the epigastric region and dysphagia. When involved in the process of overlying parts of the digestive tract, gastric lesions can be detected only with the help of fibrogastroscopic examination, as simple detection of the pathogen in the stomach contents may be the result of ingress of fungi from the mouth and esophagus.
Candidotic enteritis is characterized by frequent liquid stools of yellow and ochre color, sometimes with veins of blood. The main cause of the general condition is the loss of fluid and electrolytes. The process is bought by a specific treatment, although sometimes the disease is resolved spontaneously. Fatal outcomes in newborn children have been described, and small bowel ulcers have been detected without any manifestation of oral candidiasis,
Biliary tract lesions are extremely rare and are manifested by hectic fever, liver disease, jaundice and itching.
Anorectal candidiasis is accompanied by pain and a burning sensation, which is intensified by defecation. The mucous membranes are red, swollen. This form of candidiasis in children is constantly combined with erythema of the perianal skin.
When the disease turns into a chronic form in a number of patients the process is not limited to the mucous membranes of the oral cavity: develops heilitis, esophagitis, onychia and paronichia, and in girls - genital lesions. This form of disease due to the spread (dyssemination) of fungal lesions is called chronic generalized skin-mucosal condosis.
The course of the disease is very long, with periodic exacerbations, despite modern methods of treatment.
The prognosis in most cases is serious. Wasting develops even in a very caloric diet. In this condition, the joined intercourse disease may lead to death.
Visceral (systemic) candidiasis
Cases of common combined candidiasis with internal organs lesions, with the development of yeast sepsis began to be recorded in all countries due to the widespread use of antibiotics to treat a variety of diseases. It is believed that in the pathogenesis of visceral candidiasis is important phenomenon of dysbacteriosis, which is characterized by oppression (action of antibiotics) of the vital functions of gram-negative sticks and coccuses, which are antagonists of yeastlike fungi of genus Candida in the body of a healthy person and deter their development. Broad spectrum antibiotics (penicillin, streptomycin, biomycin, synthomycin, terramycin, etc.) and especially their combinations give the greatest importance to the development of dysbacteriosis. The use of antibiotics violates the vitamin balance in the patient's body (for example, suppresses E. coli, which takes an active part in the synthesis and replenishment of various vitamins), vitamin deficiency occurs, which contributes to the development of candidiasis. It is believed that antibiotics directly stimulate the development of yeastlike fungi. Currently, corticosteroids and cytostatics also play a role in the pathogenesis of visceral candidiasis, although the mechanism of their action leading to candidiasis has not been sufficiently studied. Apparently, in the pathogenesis of visceral candidiasis the disassembled causes matter, with the prevalence of dysbacteriosis factor in some cases, and vitamin deficiency in others, etc.
Clinic and flow. In visceral candidiasis, the most frequently affected are mucous membranes of the respiratory tract, gastrointestinal tract, genitourinary organs. Yeast affections of cardiovascular and nervous systems, kidneys, liver, spleen, bronchi and lungs (pneumonia), brain tissue, heart muscle, blood vessels and other organs are described. Visceral candidiasis can lead to a septic state, which sometimes occurs without previous damage to internal organs.
Candidotic septicemia develops as a result of exogenous or endogenous penetration of the causative agent in the blood. The main symptoms are fever: a sudden rise in temperature to 39-40 ° C, possible feverish waves of short duration, repeated 1-2 times a day. Some patients have no febrile attacks against the background of fever.
Without treatment, the general condition of the patient worsens. Repeated attacks of fever exhaust the patient, whose skin becomes earthy. Progressive illness leads to loss of consciousness, but such an acute start is not observed in all patients.
The urgency of the problem of generalized candidiasis can be judged by the results of hemoculture studies at the Mayis Clinic (Rochester, USA): from 1982 to 1990, Candida mushrooms were isolated from the blood of 226 patients, including 101 patients with C. albicans. According to the Clinical Center of the National Institutes of Health (Bethesda, USA), in 1984 Candida mushrooms were the 4th most frequently excreted from hemocultures, giving way to staphylococci (epidermal and gold) and Escherichia coli.
Speed and candidiasis
Since AIDS caused by human immunodeficiency viruses (HIV-1 and HIV-2) is characterized by T-helper lesions, it leads to severe disorders of both cellular and humoral immunity. The symptoms of developed immunodeficiency are extremely diverse and may include lymphadenopathy, pneumonia caused by Pnetanocystis carinii, tuberculosis, toxoplasmosis, generalized infection with SARS, cytomegalovirus and herpetic lesions, unusual tumors (Kaposi sarcoma, primary brain lymphoma), fungal infections.
Mycotic lesions are registered in 58-81% of AIDS patients. Mycoses may develop not only during the manifesto period of AIDS, but even during the latent stage of HIV infection. In the structure of mycotic complications, candidiasis accounts for 80-90% of cases. Posthumously dysfunctional candidiasis is detected in 20% of AIDS patients who have died.
According to the Center for Disease Control (USA), 3170 AIDS patients were registered between May 1993 and June 1994, including 41.8% of oral and pharyngeal candidiasis, and 9.4% of cases of candidiasis esophagitis. According to other data, Candida esophagitis is found in 35% of HIV-infected individuals.
French researchers have found candidiasis in 41% of HIV-positive individuals. A slightly lower incidence of candidiasis (27%) was found in a similar category in the Central African Republic.
Women infected with the virus often have candidiasis vaginitis along with oral mucous membranes: 23% of the women surveyed had this form of fungal disease in particular.
In comparison with other immunodeficiency conditions, candidaemia, despite intensive colonization of the oral and pharyngeal mucous membranes, is rarely encountered against the background of AIDS and only in the terminal stage of the disease. The causes of dysemia are neutropenia or antibacterial therapy; its development is facilitated by intravenous catheters.
In the gastrointestinal tract, the infection spreads "along the length". The role of C. albicans in the origin of persistent diarrhea in AIDS patients is known, as often in repeated bacteriological studies it is not possible to identify any causative agents other than this fungus. Pulmonary lesions occur as a result of aspiration of the fungus from the mouth or hematogenic proliferation and are limited in the form of lesions of individual bronchioles or small alveoli. The mushrooms may infiltrate the tissue as secondary pathogens, penetrating through erosion caused by herpetic infection. In general, candidiasis lesions of the respiratory system are rarely recorded.
Hematogenous disruption leads to the development of multifocal abscesses in the kidneys, heart and brain. It reveals grouped or lying separately hyphae and blastonidium fungus, surrounded by neutrophils, fibrin and cell detritus. Epithelioid and giant cells are absent in the lesion foci, making it difficult to determine the timing of the infection based on inflammation phases.
Candidosis of mucous membranes with an unsuppressed pathogenetic background (no history of therapy with cytostatics or antibacterial antibiotics, normal endocrine status) is a typical marker of AIDS. While 20% of patients who have died of AIDS are found to have had a disseminated candidiasis at autopsy, the majority of patients die from another infection - pneumocystic pneumonia, CNS cryptococcosis, toxoplasmosis, generalized infections caused by cytomegaloviruses or SARS, and Kalosha sarcoma.
In HIV seropositive individuals, the frequency of sniffing of Candida fungi on oral mucosa has increased (77.8%). At the same time, almost half of mykonositors (in 49.1% of cases) show mycelial forms of fungi without any clinical manifestations of candidiasis.
Candidotic esophagitis is considered an important clinical sign of AIDS and is included in the list of the major AIDS marker diseases. In most patients, esophageal candidiasis is manifested clinically in the form of dysphagia and chest pains, and combined with candidiasis of the mucous membranes of the rx cavity, asymptomatic diffuse lesions are also possible. Symptomatic candidiasis-free esophagitis without concomitant candidiasis of oral mucous membranes has been described.
Thus, candidiasis of the oral cavity, esophagus and vagina can develop both in the prodromal period and during the manifesto stage of AIDS.
Candidotic lesions in HIV-infected individuals are peculiar and differ from the manifestations of chronic skin-mucosal candidiasis. Attention is drawn to the high incidence of lesions of the oropharynx and esophagus and much less common vulvovaginitis, as well as the absence of the mycotic process on the nails.
Laboratory diagnostics
Polymorphism of clinical manifestations of candidiasis determines the variety of pathological material to be tested in the laboratory. Depending on the nature and localization of lesions, for laboratory analysis take sputum, scrapes from the skin or mucous membranes, nail scales, blood, liquor, urine, bile, faeces, closed cavity points, separated fistulas, biopsy and sectional material.
First, native material (except for blood) is examined, with liquor, urine and bile subjected to preliminary centrifugation (1500-2000 rpm, 10-15 min). The preparations are prepared in 10-20% alkaline solution with low heating. Then a microscopy of painted preparations (1% solution of methylene blue, gram, hematoxylin + eosin, etc.) is conducted. Detection of filament phase of the causative agent (mycelium or pseudomycelium) is an important evidence of candidiasis. The number of yeast cells in each field of vision (on average) serves as a guideline for the preparation of serial dilutions for quantitative sowing to dense nutrient media: single cells in the field of vision at high magnification of the microscope (X 400) indicate their content of the order of tens of thousands in 1 ml of the studied material.
Dilutions of pathological material containing normal microflora (sputum, faeces, urine, bile, etc.) are prepared in liquid wort or Saburo liquid medium and sown a certain amount (0.1-0.2 ml) to similar dense media. To inhibit the growth of contaminating bacteria in the medium add antibiotics most often penicillin and streptomycin - 50-100 units/ml or 0.05 % chloramphenicol.
Species identification of isolated cultures is the most important criterion for diagnosis and has a complex character, including the study of the appearance of the colony, the enzymatic activity and assimilation ability of the strain, the type of filamentation, as well as the nature of growth in a liquid nutrient medium (the presence of a surface film, a ring rising on the tube wall above the surface of the medium, etc.).
Because of the sharp predominance of S. albicans in patients and mykonosexuals in the grown culture, first of all, reveals the presence of a characteristic morphological feature of this species - chlamydospora. For this purpose, intermittent bar sowing on rice agar is performed, part of sowing is covered with flamboyant cover glass. Sowing is incubated at 37 ° C or 22 ° C. The vast majority of strains of C. albicans form chlamydosphores after 12-24 hours, less often - after 48 hours. Identification of chlamydospores allows to identify the culture as C. albicans and not to conduct further research.
Chlamydospor cultures are studied by a set of features. The enzymatic activity is determined on ordinary media of "motley row" or in yeast autolysis, in which the concentration of carbohydrates should be 2%.
In the last decade, a number of automated systems for species identification of fungi of the genus Candida have been developed, based on the determination of the assimilation ability of the studied cultures. Each well contains a specific source of food, crops are incubated at 30 ° C for 24 hours. The turbidity of the medium indicates the assimilation of this food source, the results are recorded photometrically. With the help of a computer according to the numbering-code principle the species definition of the strain is performed.
Serological tests. The agglutination reaction (RA) was widely used in the diagnosis of candidiasis until the 1960s. It differs in simplicity of setting, possibility to use autoshtame as antigen. Denaturation of the fungus is achieved by preheating at 70 ° C for 1 hour or formalin (0.5%, 12 hours).
The indirect immunofluorescence reaction (IRIF) is of high diagnostic value. 1-2 day culture of the autoshtam and antibodies - the patient's serum are used as an antigen. In practically healthy persons, antibody titers in RNIF vary from 0 to 1:40, and in most cases they do not exceed 1:10-1:20. Titers 1:80 and more are diagnostically significant. In superficial candidiasis, antibody titers in PHIF do not exceed 1:160; in chronic skin-mucosal candidiasis, especially in cases of granulomatous affection, they range from 1:160 to 1:1280; in gastrointestinal, lung, urinary and sepsis infestation -1:160-1:320; in candidiasis endocarditis - 1:1280.
The diagnosis of candidiasis also uses the indirect hemagglutination reaction (PHHA), using erythrocytes sensitized by the extract of destroyed fungus cells as a diagnosis. Positive RHGA was detected in 75% of the control group at the average titre 1:16 with a spread from 0 to 1:32. At examination of 36 patients with visceral candidiasis, antibody titer in RHGA was 1:320-1:640; according to other data, the average titer was equal to 1:256 with the spread from 1:64 to 1:512. In local lesions of mucous membranes (e.g., candidiasis vaginitis), lower antibody titers were noted: with an average value of 1:77, the spread was 1:4-1:256.
The serum definition of circulating candidiasis antigens, especially somatic antigens, is significantly more valuable than antibody titration. For these purposes, immunochemical and immunoradiometric methods are used to detect the fungus antigen nanogram fraction. The problem is complicated by the possibility of circulating immune complexes in the serum, where antigenic determinants are blocked by antibodies. In the case of polysaccharide antigens, it is suggested that such immune complexes be destroyed by short-term boiling. In case of disseminated candidiasis, mannanum can be detected in 60-70% of patients.
Serological reactions should combine several types of studies using homologous type antigens. The increase in antibody titers indicates the activity of the candidiasis process.
Treatment
The nature of therapy for candidiasis depends on the form of the disease and its pathogenesis. In case of surface lesions of the skin and mucous membranes antiseptics (borax solution, Castellani paint) are used. Some forms of superficial candidiasis (for example, interfinger yeast erosion of hands) are cured after elimination of factors favorable for their development (maceration of epidermis with water, action of acids and alkalis, syrups, etc.) and prescription of external remedies, among which the best for treatment of yeast lesions are 1-2% aqueous or alcohol solutions of aniline paints: gentic violet (crystal violet), methylene blue. Prescription of aniline paint prepared on alcohol: Rp. Gentianviolet, seu Methylenum coeruleum 0.4 Spiritus vini rec-tif. 40% 20,0 MDS.
In case of common and persistent forms of skin candidiasis and visible mucous membranes, if possible remove or reduce the detected adverse external and internal factors, prescribe antibiotics against yeast - nystatin or levorin in daily doses of 2 000 000-3 000 000 units (with division of the drug dose into 3-4 doses) during 14-17 days depending on the nature of the process. The treatment with nystatin and levorine is combined with the prescription of B vitamins, ascorbic acid, rutin, and in addition, vitamin A concentrate for children. Amphotericin B is an effective anti-yeast agent for systemic and chronic skin and mucosa candidiasis.
Amphotericin B is administered intravenously in drops at the rate of 250-500 units per kilogram of body weight during 4-8 weeks; a course dose of 1-2 million units. The antibiotic is toxic to the macroorganism and often its administration leads to the development of adverse reactions. Nephropathies are especially common, and less often - the oppression of hemopoiesis, acute liver failure or allergic reactions.
If the drug is poorly tolerated, its dose is reduced, it is administered in short cycles of 5-6 days (4-6 cycles with intervals of 5-6 days) or 2-3 times a week.
In candidiasis of the intestine and urinary system is effective mycogeptin, administered orally to 250000 units 2 times a day for 1.5-2 weeks. After a weekly break, the treatment course is repeated.
It is effective in the treatment of various forms of Mycosystemic candidiasis. (fluconazole), produced by "Gedeon Richter". Daily dose of the preparation is 50-100 mg for 7-14 days, sometimes up to 30 days.
The duration of the treatment course in case of superficial Candida-Dose lesions of skin and mucous membranes is 1-4 weeks. In case of disseminated visceral and chronic skin and mucous membrane candidiasis, the preparation lasts from 3-4 weeks to several months. Long-term remission is achieved even in those patients who have developed relapses after amphotericin B treatment. Mycosyst is contraindicated in pregnancy, as well as in liver and renal failure, the drug is virtually non-toxic.
The drug is discontinued a week after the disappearance of clinical manifestations of mycosis. To improve the absorption of mycosist, it is recommended to take it with meals.
Good results are noted in the treatment of patients with various clinical forms of candidiasis with Diflukan (vial ash), which is available in tablets of 100 and 200 mg or in vials (for intravenous injections) of 200 and 400 mg. Half-decay period of the drug is 30 hours, so take Diflukan once a day. The preparation is well absorbed, its concentration in saliva and sputum is the same as in plasma, and in cerebrospinal fluid - 5-9 times higher than in plasma. The indications for diflukan are surface and deep forms of candidiasis and cryptococcosis.
Diflukan treatment has also been shown to work well in HIV-infected candidiasis patients, although the incidence of adverse reactions has been somewhat higher.
The emerging data on the drug resistance of C.albicans to fluocolanazole (Diflukan), itraconazole and other drugs, especially in HIV-positive patients, require the determination of the drug sensitivity of pathogens to antifungal antibiotics.
In addition to etiotropic therapy, drugs are used to correct the pathogenetic background on which candidiasis has developed (dysbacteriosis, endocrinopathy, neutropenia, hemolytic conditions, etc.). In immunodeficiencies, pathogenetic treatment is determined by the nature of the immune system defect. In case of selective anergy to fungus antigens, 200-500 ml of blood is transfused from an immune donor or a transfer factor, which is a low-molecular (2-7 kD) dialysis of immune lymphocytes, is injected. Passively transmissible hypersensitivity of the delayed type persists on average up to I year.
Optimal clinical effect in the treatment of candidiasis patients is achieved by a combination of pathogenetic and antimicrotic therapy.
Approaches to treatment of acute candidiasis vulvovaginitis and its chronic recurrent forms are different. In the treatment of acute KB, preference is given to local therapy in the form of ointments, creams, aerosols, tablets and suppositories containing local antimicrotic drugs. Among these compounds, azole derivatives have established themselves as a means to obtain a therapeutic effect in a shorter time.
Schemes of local application of the above antimicrobial agents can be presented as follows.
Klotrimazole: 2% ointment (5 g) - 7-14 days; 10% ointment (5 g) - once; candles 100 mg - 1 candle 7 days or 2 candles - 3 days; candles 500 mg - once.
Myconazole (dactarine): 2% ointment (5 g) - 7 days; vaginal suppositories 100 mg - 2 suppositories 7 days each; vaginal suppositories 200 mg - 2 suppositories 3 days each; vaginal suppositories 1200 mg - one time.
For external application 1% terbisil cream is used 1-2 times a day for 7-10 days.
Antimicrotic preparations of a wide spectrum of action are also highly effective, such as pymafucine (natamycin) and pima-fucort. The course of treatment with pymafucine is 3-6 days. Pamafuccin is used in the form of tablets or candles. Vaginal candles are prescribed at night (1 candle), tablets (0.025 g) - 1 tablet intra-travaginally 4 times a day. Pymafukort in the form of ointment is applied to lesions with a thin layer 2-3 times a day for 1-3 weeks.
A good therapeutic effect is achieved by using a combined preparation of polygenax produced by the French company "Innotec International". Each granule of polygenax contains antibacterial antibiotics (neomycin sulfate - 35000 ME and polymyxin B sulfate - 35000 ME) and antifungal mystatin (100 thousand ME). Vaginal granules are injected at night for 1 piece for 6-12 days (menstruation is not a contraindication to start or continue treatment).
Polygynax is used to treat vulvovaginitis, vaginitis and cervicitis of bacterial or mycotic nature. Polygynax produces particularly good results for mixed infections. However, a wide range of the drug action does not exclude the need for preliminary laboratory confirmation of the etiology of the disease.
For successful treatment of chronic recurrent KB it is necessary to analyze possible causes of relapse, among which the most common are endocrinopathies, hormone-dependent diseases of the genitals, chronic posthemorrhagic iron-deficiency anemia, hormonal contraception, as well as inflammatory processes supported by the presence of trichomonas, chlamydia or gardennerell. In chronic KB endogenous nature, high insemination of vulva, urethra, perianal and intestinal fungi leads to frequent complications. The effect of treatment is possible in complex therapy, aimed primarily at eliminating the causes of relapses. Often, the effect can be achieved only with prolonged therapy (at least 6 months). Oral clotrimazole or ketoconazole in a dose of 100 mg per day is prescribed.
The final stage of complex treatment is the use of candles or suppositories with lactobacilli or bifidobacteria. The use of biopreparations also exists as a method of treatment of acute KB, regardless of the state of normal vaginal microflora. It has been shown that Lactobacillus case/ var. Rhamnosus candles containing 0.5 g of lyophilically dried cells (10s CFU) provide active colonization of the vaginal mucous membrane with appropriate lactobacillus lactobacteria, which are detected in the secrets within 7 weeks after the S-day treatment.
In case of vulvovaginitis caused not by S. albicans but by other types of Candida fungi, oral application of imidazole and local application of fluorocytosine or glycerine sodium tetraboragum solution are recommended. It was found that 80% of KB patients have intestinal dysbiocenosis, therapy of which promotes normalization and vaginal biocenosis.
Prevention of candidiasis
Timely detection and treatment of yeast lesions, especially of oral mucous membranes, in children and caregivers is the prevention of mass candidiasis in children's groups (thrush, jams, yeast intrigue of newborns). In newborns, the prevention of thrush infections is associated with measures to sanitize pregnant and nursing mothers and prevent people suffering from yeast infections from taking care of their children. Sick children should be isolated from healthy ones. In the prevention of children's disease, rational nutrition, hygienic care, and disinfection of care items and underwear are of great importance. It should be recalled those exogenous and endogenous factors that contribute to the development of candidiasis and strive to eliminate them. Thus, antibiotics and corticosteroids should be prescribed against the background of saturation of the patient with vitamins, carefully and regularly monitor the oral cavity, as the appearance of white plaque is often the first signal of visceral candidiasis.
Control over compliance with production technology is a preventive measure of interfinger yeast erosion of the hands of workers in canning and fruit and vegetable industries, where it should be excluded maceration of the epidermis with water, acids, fruit syrups, to combat injury.
Treatment of diabetes and obesity in persons with impaired metabolism, diseases of the gastrointestinal tract, vegetoneurosis, general strengthening therapy for weakened patients, people who have suffered from severe infections, the elimination of vitamin balance disorders - all this is a prevention of the development of surface and systemic candidiasis. In order to prevent candidiasis, these patients are recommended vitamins, especially group B, and those receiving large doses of antibiotics and corticosteroids - a preventive course of nystatinotherapy.
Dermatophytosis - combine a group of fungal diseases caused by fungi dermatophytes, which have tropism to the skin and its appendages - hair and nails. Nowadays, dermatomycoses are called skin mycoses, trichomycoses - lesions of the hair follicle, hair, onychomycosis represent lesions of the nail plates.
Dermatophytes - fungi of the genus Trichophyton, Microsporum and Epidermophyton - are the agents of dermatophytosis. According to different data, these infections affect from 10 to 40% of the world's population. Out of more than 40 known types of dermatophytes in our country, three are most often found - Trichophyton ru-brum, Trichophyton m entagrophytes var. Interdigitale, Microsporum canis, less often Epidermophyton floccosum.
Pathogenesis and immunity
The main pathogenic property of dermatophytes is their ability to destroy keratin with the help of their enzyme - keratinase. Thus the mushrooms penetrate into the stratum corneum, the horny structures of hair and nails.
In the incubation period, the mushrooms are multiplied and colonized in the horny layer. This is followed by an infestation, ie the introduction of a colony of mushrooms in the layers of the epidermis. However, the mushrooms usually do not penetrate deeper than the epidermis, because the protective factors of the macroorganism - phagocytosis, opsonating antibodies, complement, etc. - act.
Inguinal epidermophytia (Epidermophytia ingvinalis), synonymous - epidermophytia of large folds, tinea cruris.
Etiology The disease is caused by pathogenic anthropogenic fungi Epidermophyton floccosum.
Epidermophyton floccosum as a mycosis pathogen accounts for not more than 1.5% of all dermatophytic pathogens.
Inguinal epidermofitiya is predominantly male at a young age. The reason of such sexual and age predisposition, apparently, lies in anatomical and physiological peculiarities - hip traumatization during its friction with scrotum, special composition and ph perspiration secreted by apocrine glands of femoral and genital area, whose function is more pronounced in men, especially in young age.
Infection occurs through direct transmission of the pathogen from a sick person to a healthy person, as well as through objects and clothing, the surface of which is contaminated with mushroom flakes of skin of a sick person. Infection is also possible through medical instruments and objects - liners, urinals, underwear, towels, thermometers, if they were not properly disinfected.
The emergence of the disease is facilitated by increased sweating, wearing clothes made of synthetic fabrics, which impede the aeration of the skin and sweat evaporation, carbohydrate metabolism disorders, vegetative disorders. External factors are important in the spread of infection, first of all, increased temperature and humidity, so the incidence of large folds of mycosis increases in spring and summer, as well as in tropical and subtropical climates.
Clinic. Inguinal epidermophilia usually begins acutely and in the absence of rational treatment may turn into a chronic form with exacerbations in summer.
The disease, as a rule, begins in the inguinal folds. Dermal process is characterized by the appearance of poorly peeling, sharply limited inflammatory spots of pink or red, which are increased by peripheral growth. In the central part of the rashes there is a resolution of the pathological process in the form of peeling. The peripheral part is represented by a well expressed edematous solid or intermittent roller of bubbles, erosions, scales, crusts, and nodules, sometimes pustules. The inflammatory process is sometimes accompanied by soaking, imitating eczema. In this regard, the disease was first described by Hebra (1860) under the name "fringed eczema", eczema marginatum and only later was established its fungal nature.
In the central zone of process resolution and outside the main focus may appear additional foci of lesion (elimination).
As the peripheral growth of rashes merge with each other and form ring-shaped, garland-like shapes that extend beyond the folds.
Subjectively, the patients are concerned about itching, burning, painfulness, especially when moving.
Much less frequently involved in the process are other large body folds: the area of the crotch, armpit folds and folds under the mammary glands. Sometimes, the centers of mycosis may be located on the skin of the body and limbs.
The course of mycosis may be complicated by the addition of secondary piococcal or candidiasis infection, which is often observed with glucocorticoid ointments. The clinical picture is dominated by the phenomena of pustularization in the foci of lesions, sputum and maceration.
Differential diagnosis. Streptococcal intertrigo develops in large - armpit, inguinal, intercostal and under the mammary glands folds, as well as in the interfinger intervals in the form of flinthenes, which quickly open with the formation of large erosive surfaces. The erosions are bright red, have clear coarse-festoon borders, and are bordered by a narrow whisk of a detached epithelium. Patients are worried about itching and burning. In the depth of the fold, there are often deep painful linear cracks.
Candidate intertrigo can develop in any folds of the body - in the inguinal and hip, buttocks, armpits, under the breast of women, in the folds of the abdomen and neck of obese people, less often in the folds behind the auricles, interfinger intervals. There is the appearance of surface bubbles and pustules, which quickly open, turning into prone to peripheral growth and fusion of erosion. Erosions have a bluish red color, moderately wet surface, polycyclic edges, fringed by a whisk of swollen macerated epithelium. At the depth of the fold usually appear linear cracks, clusters of whitish porridge mass of macerated horn layer of the epidermis.
Inverse psoriasis, located in the inguinal, intercostal, armpit folds, in the navel area, due to the absence of the characteristic silver-white peeling, may acquire atypical appearance. However, the process is represented by flat rounded papules and plaques of polycyclic outlines, with clear boundaries. When scraping can get symptoms of the psoriatic triad: stearic spot, terminal film and blood dew). In addition, the patient is carefully examined to identify lesions of the skin, which have a typical appearance, in other areas of the skin.
Diagnosis is based on the characteristic clinical picture, as well as the results of microscopic and cultural examination of the infected material. Skin scales, better from fresh but fully developed foci, should be examined for fungi. Skin scales should be scraped off the periphery of the focus with a scalpel.
Microscopic examination of pathological material for fungi is performed in native preparations. In the preparation of unpainted drugs for a clearer identification of the elements of the fungus make the clarification of pathological material 10%-20% caustic solution (KON or NaOH) for 10-15 minutes. Microscopic examination is performed on an ordinary laboratory microscope without immersion. To increase the reliability of the analysis it is recommended to test several drugs. Septized branched short (2-4 microns) mycelium of the fungus and a chain of rectangular arthrospores are detected in the preparations.
As a highly sensitive and specific diagnostic method, a cultural test should be performed independently of the microscopy results. Sample material shall be sown with at least 4-5 tubes. Saburo medium with 2-4% glucose solution or wort agar containing antibacterial and anti-candidase agents (penicillin 50 µg/ml, streptomycin 50 µg/ml, cyclohexamide 0.1-0.5 mg/ml) is used. Seeds are incubated at 22-30°C. Appearance of epidermophytes growth is observed from the 4th to 12th day of incubation. E. floccosum culture has a characteristic view with microconidia, located in groups in the form of banana bunches. Absence of growth during 30 days allows to consider the result of the study negative.
Treatment is carried out mainly by external means, in persistent cases systemic antifungal drugs are prescribed.
In case of island-inflammatory phenomena desensitizing and antihistamine preparations are prescribed, external water solutions of anti-inflammatory and disinfectants in the form of lotions - Alibura liquid, 0,25% silver solution, 1-2% resorcin solution and others. After the disappearance of acute inflammation phenomena, water and then alcohol solutions of aniline dyes are used - 2% solution of methylene blue, gentianviolet, "Fucorcin" solution. Then, it is prescribed to lubricate the lesions with 1% iodine tincture, salicylic-benzoic iodine, 3-5% sulfur-degty ointment, fungicide means - lamizy-lom, clotrimasol, mycoseptin, herbalogen, and especially effective is the use of 1% terbisil cream 1-2 times a day for 7-10 days. A good therapeutic effect in case of acute skin condition is observed from the use of the cream "Triderm", skin lubrication is carried out 2 times a day for 7-10 days.
Dermatophytes of smooth skin include foot and hand mycoses.
The general term "mycoses of feet" refers to fungal lesions of the skin and nails of feet of any nature. They are found in about one in five people on the planet, their frequency increases with age.
There are many factors that contribute to the growth of mycosis in the feet. These include extensive exposure to pathogens in swimming pools and ponds, general aging of the population, wearing of airtight and tight shoes, increased use of antibiotics, cytostatics, corticosteroids, estrogen-gestagen drugs, diabetes mellitus, and HIV infection.
The range of pathogens of this disease is very diverse and variable: Trychophyton rubrum is 70% to 95%, Trychophyton mentagrophytes (interdigitale) - from 7% to 34%, Epider-mophyton floccosum - only 0.5-1.5%. Nowadays, yeast and mold fungi, as well as mixed fungal infection are becoming increasingly important in their etiology.
Epidemiology. Distribution is ubiquitous. The source of infection is a sick person. The disease is transmitted through close contact with the patient or through objects that he used (shoes, underwear, towel, washcloth, carpets, etc.). Infection can occur in public places (baths, showers, swimming pools, beaches), in the family and at work.
The following forms of foot mycosis are distinguished:
- Interfinger.
- Skvamoznaya.
- Dyshydrotic.
- Acute form (exudative).
Clinic. Acute forms of foot mycosis, usually caused by Trychophyton mentagrophytes (interdigitale), are accompanied by hyperemia, edema, vesiculo pustules, cracks and erosions, are painful, make it difficult to wear shoes and move, and with complications of lymphangitis, lymphadenitis, mycides - poor overall health, fever. The disease begins with an asymmetrical lesion of the interfinger folds or the arch of the foot. This lesion may exist for a long time and give exacerbation in the spring-summer period of the year. In the long course of the disease process captures the skin of the interfinger folds and the vault of both feet.
Interfinger (interfinger) form, when in III, IV interfinger folds of the feet appear redness, peeling, maceration with clear borders. Cracks are formed in the depth of the folds, which turn into erosion, fringed with a whitewashed subverted layer of epidermis. In the hot season, this form of disease may turn into dyshydrotic. In the interfinger folds, on the vault of the feet appear saga-like bubbles with a thick horn tire. The content of the bubbles in the first days is transparent, from 2-3 days - blurred due to secondary infection. Often, the bubbles, merging with each other, form multi-chamber bubbles. By the end of the week, the bubbles open with the formation of erosions fringed by a whitish horn layer of epidermis. With the progression of the disease process takes on a common character with dispersion on the side surface of the toes and palms.
Squamous and squamous hyperceratotic forms of lesions, often caused by Trychophyton rubrum, often begin with the lesion of the interfinger folds of the feet, where there are hyperemia and branched peeling. Gradually, the process spreads to the skin of the vaults and the side surface of the feet. The skin of the soles becomes stagnant and hyper-removed. Dryness and moderate hyperkeratosis, flaking in the skin furrows are noted. Dryness and hyperkeratosis may be absent, and collar-like peeling is noted on a stagnant and hyper-removed background. The lesion of the foot may be continuous, like an eyelid or an Indian stocking - "moccasin type", or in the form of hearths, spots. The process from the foot switches to the brushes. The right palm is more often struck. The skin of the palm is stagnant and hyper-removed, with branched exfoliation, whitish skin furrows, but it can be exfoliated in the form of rings, with festoon shapes. Often the process from the palm to the rear of the brush in the form of erythemato-scwamosis foci with a peripheral intermittent roller, consisting of nodules, bubbles, crusts. Often rashes are dispersed to large skin folds, then to other parts of the skin. When the mycosis of the feet and the hand is combined, this condition is called the syndrome of two feet and one hand. Along with rather superficial mycotic rashes, deep skin-subdermal nodes caused by Tr. rubrum can form. They are localized more often on the lower leg skin, less often on the face, and even less often on the scalp. In such patients, cannon and long hair like ectotrix or endo-ectotrix are often affected.
Differential diagnosis is made with eczema, deep folliculitis, inguinal epidermophytosis, neurodermitis.
The diagnosis of mycosis of the feet, hands is made on the basis of clinical manifestations and confirmed by the discovery of septized mycelium in the scrapes from the lesions and the isolation of mushroom culture. Treatment of patients with foot mycosis (MS) should be complex and include antifungal preparations for general (systemic) and external use, as well as pathogenetic agents.
Currently, practical mycology has three effective systemic antimicrobials at its disposal - azole compounds: itraconazole (orungal) and fluconazole (diflukan), as well as an allilamine derivative - terbinafine (lamisil and terbisil). These drugs have keratinotropic and lipophilic properties, they enter the corneal layer of the skin and nails quickly enough and remain in them for a long time, allowing for relatively short courses of therapy. The duration of treatment with systemic antimicrobial does not exceed 2-4 weeks. Terbisil is prescribed in a dose of 250 mg (1 tablet) per day for 2-4 weeks.
The therapy with systemic antimicrotics should be supplemented with external fungicidal-keratolytic agents. In case of squamous and hyperkeratotic forms of mycosis, it is necessary to peel off the stratum corneum (applications of 10% of milk-salicylic collodium during a week or peel-offs according to Whitefield Arievich) with subsequent use of one of the local antimicrotics 1-2 times a day until clinical manifestations of mycosis are resolved.
After that, the local antimicrotic agent in the form of 1% terbisil cream is used for another 1-2 weeks.
In exudative (interrigenous, dyshydrotic) forms, locally prescribed primaries, trays with various disinfectants, then proceed to keratolytic and antimicrotic agents. It is possible to prescribe Triderm cream 2 times a day, 7-10 days.
Pathogenetic means of therapy, on the one hand, increase the effectiveness of treatment with systemic and external antimicrobial agents of MS patients, on the other hand, reduce side effects and complications. These remedies are as diverse as the pathology against which MS occurs.
Patients with exudative forms of MS are prescribed hyposensitizers: calcium preparations, 30% solution of sodium hyposulfite - 1 tbsp three times a day, effective administration of antihis-tamin preparations, 25% solution of magnesium sulfate in the form of intravenous injections. Taking into account frequent vascular pathology, MS patients are shown angioprotectors and drugs that improve tissue trophicity: troxevasin, nicotinic acid preparations. Of physiotherapeutic procedures, we recommend inductothermy of sympathetic ganglia, electro- and ionophoresis with iodine preparations, ultrasound to the region lymph nodes. The correction of immunological disorders is the most important. For this purpose, a variety of non-specific and specific immunocorrective drugs (drugs of the thymus gland, pyrogene drugs) are used. It is expedient to combine the above mentioned preparations with adaptogens - preparations of ginseng and eleutherococcus, Chinese lemongrass and lures, sarsaparilla, dibazole and other means. To protect the membrane structures of immunocompetent cells, antioxidants are prescribed. Self-massage of the lower extremities, "stretching" spine gymnastics are useful.
Lack of sulfur and sulfur-containing amino acids is compensated by food rich in these substances (eggs, curd, herbs, and mineral waters containing them).
In order to prevent relapse and avoid contamination of the surrounding patients, the MS should follow the rules of personal hygiene. During the treatment it is necessary to wipe the inner surface of shoes once in 2 weeks with a cotton swab wetted with 0,5 % solution of chlorhexidine bibluconate. It is also possible to use 10 % formaldehyde solution, chlordezine, chlorcine, sulfochlorantine, white nirtan, catamin AB, ampholan, etc. for footwear disinfection.
Control of foot sweating is an important aspect in prevention of MS and their relapses. In case of foot sweating, we can recommend Svezheste-Amiko powder from Prizero Company, traditional remedies such as Formidron, Finish, boron-urotropine paste, urotropine solution, and others.
It is necessary to influence all the revealed pathogenetic factors, favorable for the process development. Only complex therapy with the use of general and local antimicrotics, exposure to the identified pathogenetic factors, compliance with sanitary rules can lead to sustainable clinical recovery from foot mycosis.
Tr. rubrum may cause generalized mycosis of smooth skin, less often - mycosis of large folds. In our country, this disease is called rubrophytium of smooth skin, which is the main form of tinea corporis and is often combined with mycosis of the feet, onychomycosis and sometimes palm affection. Foci are located in any part of the skin. Erythematous spots with peeling, with clear festoon borders and peripheral growth are typical.
The clinical variant of tinea corporis is most often a granuloma of Mioca and tinea faciei. The Mioca granuloma is a follicular form of rubrophytes of smooth skin, more common in women. Tinea faciei is localized on the face as erythema and peeling.
It is recommended to administer 1 tablet (250 mg) of Terbisil per day for 2-4 weeks, which will lead to a rapid regression of rashes in generalized mycosis of smooth skin. It is possible to use mycosist 150 mg once a week or 50 mg per day for 2-4 weeks.
Indispensable companion of mycosis of the feet, with a few exceptions, damage to the nails. It is generally considered to be secondary: first, pathogenic fungi affect the interfinger folds or sole, and then the nails. However, a number of authors allow the development of isolated onychomycosis when the pathogen penetrates the nail plate from under its distal, lateral, proximal edges or directly through the dorsal surface.

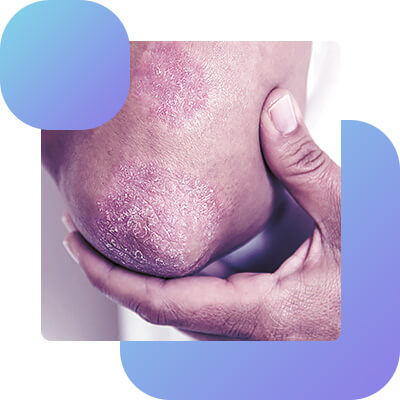


Onyhomycosis
Onyhomycosis - fungal lesion of foot nails (hands) is very common in many countries. According to WHO, foot mycosis affects from 11.5% to 18% of the world's population. This disease is faced not only by dermatologists and mycologists, but also by doctors of other specialties. At least 20-30% of patients suffering from the most common dermatoses (eczema, neurodermatitis, psoriasis), and almost every patient with somatic and neuroendocrine pathology has lesions of nail plates. At present, the increase in morbidity is due to unfavorable socio-economic and environmental conditions, the growth of immunodeficiency conditions, lack of medical care, deterioration of epidemiological control.
Etiology
About 50 species of fungi can cause damage to the nails as an etiological factor. The etiology of these diseases becomes more diverse, if we take into account the cases of micro-infection, when several types of fungi are sown from the affected nail plate. The role of many fungi as possible pathogens has not yet been established.
The main agents of onychomycosis are dermatophytes (in 80-90% of cases), among them Trichophyton rubrum, which causes damage to the nails of feet and hands, then Trichophyton interdigitale, in 10-20% of cases affecting the nails on the 1 and 5 fingers of feet and (less frequently) hands. Of trichophytons, the affection of the nails is caused by Trichophyton violaceum, Trichophyton tonsurans. There are single data on the affection of nails with Trichophyton schenleinii, Trichophyton mentagrophytes, Trichophyton verru-cosum. There are single reports of an affection of nails with fungi of the genus Microsporum gypseum. Onychomycosis may be caused by the fungus Epidermophyton flocossum, much less by yeastlike and very rarely by mold fungi. Candida spp. - is the second most common onychomycosis pathogen after dermatophytes. The share of Candida spp, among onychomycosis pathogens of feet, is small, no more than 5-10%. However, onychomycosis on the hands often causes Candida fungi - up to 40% and even 50-60% of all cases according to the results of various studies. In some countries of the world, candidiasis affects foot nails more often. Of mold fungi, Scopulariopsis brevicaulis is more common, which causes damage to the nail records mainly in elderly people.
Epidemiology
Infection often occurs in public baths, swimming pools, and shared showers. Infection may also occur in the family through household items: bath mats, washcloths, manicure supplies, shoes. It is possible to get onychomycosis at any age, including childhood, and the morbidity among children and adolescents has increased. The morbidity among different population groups is different and depends on the place of residence (country, climate, city or village), age, profession, sex and some other factors.
Much more often than the rest of the population, onychomycosis of feet can be found in miners, technical personnel of nuclear power plants, workers of metallurgical plants, servicemen and sportsmen. In these groups, the infection is predisposed to the isolation of teams assembled in a limited area, shared showers and locker rooms, uniforms, boots, etc., which are all susceptible to infection.
Onyhomycosis on brushes caused by Candida is three times more common among women, particularly among cooks, confectioners, laundries, canning factory workers who have to keep their hands in water or work with sugars. In candidiasis, fungi penetrate into the nails either from the skin or mucous membranes of the patient, or from external environment, such as food rich in carbohydrates. When the Candida mushroom affects the nail records, it first affects the nail bed, then the nail records.
Many of the mold fungi released from the affected nails live in the soil, and their spores can be found on surrounding objects.
The main agents of onychomycosis are anthropophilic fungi - dermatophytes Tr. rubrum and Tr. mentagrophytes var. The source of the causative agent for dermatophytosis of nails is usually the skin of the sickest, already infected and has dermatophytosis. With these forms of onicomycosis fungi initially affect the nails from the free edge.
Onychomycosis is not transmitted directly from person to person.
Pathogenesis
Infection of the nails contribute to injuries to nails, fractures of the bones of the feet, hands, impaired circulation of the extremities (heart failure, obliterating periarrhea, Raynaud's disease, varicose veins, etc.). More susceptible to the disease and the severe course of the process are persons suffering from severe somatic endocrine diseases, especially diabetes mellitus, as well as immune disorders of horn formation, receiving corticosteroid hormones, immunosuppressive therapy and massive antibiotic therapy.
The mushrooms cause disease by getting into the nail plate of the bed, the matrix and the proximal roll of the nail. Visible changes to the nail are the result of infection of any of these structures, and not necessarily the plate itself.
Very often fungi are introduced into the nail from under the distal (free) or lateral edge of the nail plate, the main changes occur not in the plate, but in the bed of the nail. In case of infection caused by Trbrum, the main agent of onychomycosis, the nail is preceded by an infection of the skin of the hypony-chia or the lateral fold. The mushrooms usually penetrate the nail from the focus of the fungal infection. From under the lateral and distal edges of the nail plate, the fungi penetrate into the bed of the nail. The nail bed responds to the introduction of the fungus by an accelerated proliferation. The thickening of the cornea layer at the edges disrupts the connection of the bed with the nail plate, so the early manifestation of onychomycosis is characterized by manifestations of onycholysis. Once in the nail bed, the mushrooms spread in the proximal direction. The proliferation of onycholysis leads to a detachment of the increasing surface of the nail plate. The mushrooms enter the nail plate, causing its slow destruction. They can also penetrate the matrix, leading to dystrophic changes in the nail.
In candidiasis, paroniasis, an inflammation of the proximal roll, usually occurs first. Swelling, thickening, and changing the shape of the roll result in the skin of the nail - cuticle - being separated from the dorsal surface of the plate. As a result, the mushrooms penetrate the nail matrix, then the nail plate and the bed, which may appear as onycholysis. Onychomycosis, accompanied by paronichia, is also observed in non-dermatophyte mold infections. Matrix changes in any type of proximal onychomycosis may lead to nail dystrophy, destruction and loss of the nail plate.
Clinic of Onychomycosis
Clinical manifestations of onychomycosis are diverse, which depends on the type of agent. There are several classifications of onychomycosis.
Depending on the degree of lesion of the nail plate:
- Normotrophic. In this form, the normal configuration of the affected nail is maintained for a long time, it becomes opaque, dull, yellowish color at the distal edge, with thickening in the corners of the plates due to the underlying nail hyperkeratosis.
- Hypertrophic is characterized by a thickening of the nail plate, which has a yellowish coloring at the beginning. Later, the nail is deformed, and on the nail plate there are transverse stripes, gradually open the nails at the free edge. In some patients, the nails acquire beak-shaped or change in type onychogriphosis, have a dirty gray color, fade.
- Atrophiic. In this situation, the nail plates are significantly destroyed, deformed, look as if eaten at the distal edge. The nail bed is partially exposed, covered with a layering of loose, crumbling horn masses, the nails become dull, grayish or yellowish color.
- Onycholysis. In this form, the onychomycosis of the nails thinks, separates themselves from the nail bed, loses its luster and transparency, becomes dirty grayish or yellowish. However, the matrix area retains its normal coloring.
Depending on the causative agent:
- Onyhomycosis caused by Trichophyton rubrum affects more frequently several nail records. Disease on the toes of the feet begins with the appearance of yellow stripes at the side edges of the plates. On the brushes, they appear in the center of the nail plate and their color is lighter - whitish or grayish, the nails become opaque. Children have some features: the surface of the nails is rough, the configuration can be changed, the plate is affected at the distal edge, and hyperkeratosis is rarely observed under the nail.
- Onyhomycosis caused by Trichophyton interdigitale is more often observed normotrophic shape of the lesion, in the thickness of the plate, in the center of it appear spots or stripes of bright yellow color, sometimes there is a thickening of the nail at the free edge, deformation of the plate, which looks as if it is edible.
- Onychomycosis caused by anthropophilic fungi (Tr.violaceum, Tr.tosnurans, etc.) is usually observed when the scalp and smooth skin are simultaneously affected. In superficial trichophytosis more often the disease begins with the lesion of the nails on the hands, later involved in the process and the nails of the feet. At the distal edge and on the side parts of the nails there are spots or stripes of grey color, the plate thickens, grooves appear, the nail begins to crumble.
- In onychomycosis caused by yeastlike fungi of the genus Candida, the lesion begins more often with the area of the nail roll (back or side) mainly to the fingers. The rolls thicken, become swollen, hyperemic, silver scales are visible along the edge, the epiphanychion disappears, painfulness occurs during palpation, sometimes a drop of pus can be separated. Fingernails become uneven, they have transverse grooves running parallel to the back roller, sometimes the plates break in the proximal area. However, these changes in the nail plate are due to trophic disturbances in the area of the roll. In case of candidiasis, the nail thinns more often in the area of lateral edges, less often in the distal part, and does not grow to a bed of yellowish color. It may be a nail plate affection without a nail roll.
- Onychomycosis caused by zoophilic trichophytes and microsporums is extremely rare. The clinical picture is reminiscent of onychodystrophy: first, leukonychia is observed, then there is a change in the configuration of the nail, then - the destruction of the plate from the distal edge or proximal. They do not grow to the bed, become yellowish, but may be of normal color.
- Onychomycosis caused by mold fungi, as a rule, develops secondary against the background of the primary onychomycosis of different etiologies. The lesion is superficial. The color of the nail plate varies depending on the type of pathogen: it may be yellow, green, blue, brown and black:
Depending on the localization must be distinguished:
- Distal-lateral podnogtevaya form - the most common. In this case, the lesion of the nail begins with the edges of the nail bed. First, you can observe onycholysis at the free and side edges of the nail plate: the nail loses its transparency, becomes white and yellow, the edge of the nail is uneven, crumbling, thinning. In some cases, the footsteps develop hyperkeratosis. The final stage of distal-laterial form is the defeat of all the visible part of the nail plate and matrix, leading to the nail dystrophy. Older persons are characterized by a long process, with pronounced hyperkeratosis, thinning of the plate with the phenomena of onychogriphosis or coilonichia.
- Surface white form. This form almost always affects only the dorsal surface of the nail. The process begins with the appearance of white spots or stripes on the surface of the nail. Over time, the spots take over the entire plate and change color from white to yellow, ochre. You can see that the lesions are superficial by scraping them. The nail becomes loose and rough. More often white onychomycosis is observed in the area of 1 toe, less often than 5 fingers, rarely - on the hands.
- The proximal pedicel shape. In this form, first the proximal roll is affected, and then the roll and matrix of the same nail. The proximal shape is more often called Candida spp., Trichophyton rubrum. In Candida spp., Trichophyton rubrum, the process starts with paronichia. In the beginning, the nail roll turns red, it becomes painful, swollen, thickens, due to which the cuticle is separated from the nail plate, is destroyed. The course of paronichia is wave-shaped, the nail is involved gradually. The damage to the nail can be reduced to a strip of onycholysis, which begins at the edge of the nail in the half-moon area. When the matrix is involved, a different picture is observed - dystrophic changes. Clinically, this process is manifested by white stripes on the surface of the nail plate and changes in relief in the form of irregularities.
The total dystrophic form usually develops from distal, less often from proximal forms. The nail looks thick, uneven, grayish-yellow, can be partially or completely destroyed. Hyperkeratosis of the foot often develops.
Diagnosis of onychomycosis
The diagnosis of onychomycosis is established on the basis of clinical manifestations, the discovery of the fungus in the microscopic examination of pathological material and the release of fungus culture on the nutrient media.
- Microscopic examination. For this purpose, small pieces of nails, footstep corneal layers are poured in a tube with 15-20% KON or NaOH solution, left for a day at room temperature and deposited on the slide glass with a pipette, covered with slide glass and viewed under a microscope at low and high magnification. In the preparation in the presence of fungal affection is found mycelium fungus in the form of threads, which may be thin or thick, flat, branched, septicaemia or spore, groups of spore buds or mycelium with kidney in candidiasis.
- Cultural diagnosis. Seeding is done on a standard Saburo environment, often with antibiotic supplements. In the diagnosis of dermatophyte infections is used to add to the medium Saburo cycloheximide, which inhibits the growth of mushrooms-contaminants released from the air. There are ready-made commercial environments with additives of antibiotics.
Differential diagnosis: onychomycosis must be differentiated with damage to the nails in such dermatosis as psoriasis, red flattened lichen, onychodystrophy.
Treatment
There are many remedies and methods to treat onychomycosis, and all of them are directly or indirectly aimed at removing the pathogenic fungus. Egiotropic therapy is the only effective approach to treating fungal infections of the nails.
Etiotropic treatment of onychomycosis can be either local, when the antifungal agent is applied to the affected nail, or systemic, when the drug is prescribed internally. Local and systemic effects have their advantages and disadvantages, and their list of indications and limitations.
Local therapy allows you to create on the surface of the nail very high concentrations of antifungal agent. With local application of the drug is not absorbed into the blood, and this method of treatment is safe. The disadvantage of local therapy is that when the drug is applied to the surface of a nail, it does not always reach the pathogen - a fungus located in the nail bed and even more so in the matrix. In order to ensure the access of the drug to the nail plate, a variety of kerato-lithetics are used to remove the nail plate (solypod, patch containing uric acid, Mikospor patch, quinozolone patch, soda baths, varnish Butrofen and Loceryl).
Systemic therapy provides penetration of the drug into the nail through the blood, the drug enters the nail bed and the matrix. To date, there are a huge number of systemic antimicrotics ("Nizoral", "Grizeofulvin", "Orangale", etc.). The most effective systemic antimicrotics are "Lamisil" and "Terbisil", produced in the dosage of 250 mg - one tablet. Terbisil is prescribed in a dose of 250 mg per day daily. The course of treatment for lesions of foot nail plates is - 3 months, hand 1.5 months.
During the treatment it is necessary to disinfect the shoes!
Microsports
Microsporia - fungal lesions of the skin, scalp, rarely other scalp areas of the skin (beard and moustache areas), very rarely nails, as well as palms and soles, due to fungi of the genus microsporum.
Etiology. Pathogens of microspora are divided into anthropophiles (Microsporum audoinii, Mi-crosporum ferrugineum, etc.), zoophiles (Microsporum canis, Microsporum distortium, Microsporum equinum). There are also known geophilic microsporums (Microsporum gypseum), which in rare cases can be a cause of disease, but their epidemiological significance is low.
Epidemiology. Microsporia is the most frequent dermatophytosis in childhood. Adult patients are only 10-12%. Infection of children most often occurs at the age of 1 to 13 years, less often than 15 years. By the period of puberty, all untreated patients are spontaneously recovering, which is explained by changes in the composition of skin fat and the emergence of a large number of free fatty acids with fungistatic action.
Microsports is an extremely contagious disease, both for children and animals; in children's groups (schools, nursery schools, kindergartens) it can take the form of epidemic outbreaks. Microsporum ferrugineum (an anthropophilic fungus) is the most contagious and virulent. The source of microsporum infection caused by anthropophilic fungi is a sick person and the things he or she has come into contact with (hats, tissues, combs, brushes, scissors, bedding, etc.). The disease is spread in Western Europe, the United States, Japan, Southeast Asian countries, the republics of Central Asia, and Transcaucasia. Sick kittens, less often adult cats and dogs, hamsters, etc. are the main source of human infection with Microsporum canis. In 80-85% of cases people are infected through direct contact with animals or with things, objects infected with animal hair and skin scales. Infection of people from each other is rare (in 3-5 % of cases). There are two peaks in the incidence of zoonotic microsporia - at the end of summer and in autumn, which coincides with two infertility in cats, which 3% carry Microsporum canis without clinical manifestations. The disease is common in many countries; in our country it is the main form of microsporia.
Clinical manifestations of the disease develop after the incubation period, which in microsporia caused by Microsporum ferrugineum lasts 4-6 weeks on average, Microsporum canis - 5-7 days.
Clinic. Initially, the pathogen is introduced into the corneal layer of epidermis surrounding the hair follicle, from where it enters the hair. Around the hair is formed a slightly oedematous erythematous spot, which gradually increases in size, capturing more and more skin areas of the scalp. Inflammatory changes in the lesion foci are poorly expressed.
In clinical manifestations, the microspore is divided into the superficial microspore of the scalp and the superficial microspore of the smooth skin. In some cases, a deep (purulent) form of microsporias can be found.
In the superficial microsporius of the scalp (Dermatophytosis of the scalp, tinea capitis) there are usually only single lesions of the correct round shape and relatively large size (on average from 2-5 cm in diameter), Always sharply delineated, with no tendency to merge with each other, covered with a significant amount of branched grayish-white scales, as if sprinkled with flour, sometimes on the periphery of the centers may be located small screening, diameter up to 1-2 cm. The most characteristic clinical feature is the presence of completely broken hair in the hearth, with the latter protruding 4-6 mm above the level of the surrounding skin, as if cut, corresponding to the name "ringworm". The inflammation is usually small: the skin in the area of the centers is slightly hyperemic and somewhat swollen. Possible exudation with the formation of crusts, the appearance of papules. At the base of the hair often noted whitish ring-shaped scales, surrounding them as a cuff. Hair from the centers of dull, brittle, light gray color, at the base of the hair is dressed in a white cover. At the beginning of the disease, and sometimes in developed cases, along the edge of the lesions, the hair is very easy to pull out, and on their root part is found whitish color plaque, especially expressed in the follicular funnel, such hair looks like a rolled umbrella; there is also some resemblance to a match, one end of which was covered with glue and then dumped in the sand. It is difficult and unlikely to establish the dependence of the clinical picture on the Microsporum, and it makes sense to identify any clear clinical form of microsporia.
Surface microsports of smooth skin (Dermophytosis of smooth skin, tinea corporis) is characterized by the appearance of pink spots on the head, forehead, face, neck of round or oval shape from 0.5 to 2-3 cm in diameter, resembling medallions. The abundance of centers (up to 30 and more) on the closed and especially open parts of the skin is typical for microsporia caused by Microsporum canis, and is often explained by direct contact of the child with a sick cat. In the peripheral area of the spots, there are bubbles that quickly dry out into crusts, and the central part of the spots is covered with scales. Due to the centrifugal growth of the centers (with simultaneous resolution in the center), there are ring-shaped figures with the formation of double and even triple "rings", i.e. lesions of the shape of "iris". There is no skin atrophy.
The peculiarity of this microspory is also the high incidence of cannon hair disease (up to 65.8%). Frequently, the affected cannon hair is found within the erythemato-scumosis foci of smooth skin. The location of the fungus in the cannon hair loses the features inherent to the microsatellite, the mosaic arrangement of spores is lost. Microscopic examination of the hair, as well as examination with a fluorescent lamp reveal a delayed microspore of cannon hair even a few months after the apparent cure of the microspore of smooth skin.
This is a deep (suppurative) form of microsporiasis. In rare cases, Microsporum canis or Microsporum gypseurn (Microsporum gypseurn) causes lesions on the head that resemble the suppurative form of trichophytosis (kerion), and on smooth skin, the infiltration form. Island-inflammatory reaction and purulence is not so much due to the properties of the microsporum, as a secondary microbial infection, complicating the underlying disease. Within large foci of surface microsporia, deep folliculitis with rapidly forming massive crusts and accumulation of pus beneath them occur.
Clinical manifestations of secondary allergic reactions - microsporids, are very diverse and may resemble different dermatoses. However, they are somewhat rarer than similar rashes in other mycoses, as microsporia is less likely to cause acute sensitization of the body to fungi and their products.
Laboratory diagnostics of microsporia. The material for laboratory and diagnostic testing in microsporia is hair, crusts, skin and nail scales. In flakes, the fungus occurs in the form of rather thin branching mycelium threads with rare partitions. Important importance is attached to the right choice to study the affected hair. Microsporia is characterized by broken hair at a height of 4-6 mm, with a characteristic whitish "muff" of the surrounding hair spore clusters. The affected hair in microsporia has a characteristic microscopic picture: small spores surround the hair at the base, closely adjoining each other, they resemble their mass "mosaic". Along with spores, sometimes there are septumized mycelium threads.
Several pathogens cause micro-disputation, some of which affect only humans, others - animals and humans. In microscopic examination of the hair is not possible, to determine the type of the causative agent and make an idea of the path of infection. Receiving and further study of cultures becomes epidemiologically important.
Microsporura canis, which affects cats and dogs that can infect humans, gives on Saburo environment round, wide, fluffy, gray, sometimes yellowish-pink with concentric circles of the colony. Mature cultures can be mealy, bumpy in the center. The back side is dark brown or orange.
The second place in the frequency of lesions is occupied by anthropophilic rusty microsporum ferrugineum. The disease is transmitted from a sick person to a healthy person. Mycelium branched, rarely septic, sometimes with scalloped organs. Colonies polymorphic, leathery, slightly domed with radial folds. The characteristic color of the pigment, which gives the environment a rusty shade, defines the species name of the fungus.
Geophilic fungus (Microsporum gypseum) affects horses, dogs, cats and humans. Septized mycelium, rocket-like. Colonies are flat, flat, velvety in the beginning, later mealy. The edge of the colonies is white, a small pinkish-yellow tint appears to the center. The back side is sometimes with brown spots.
Luminescent study. Hair affected by microsporia may be detected in ultraviolet rays passed through the Wood filter (glass containing nickel oxide) in a dark field. They fluorescence with a green glow.
Differential diagnosis. The scalp microsporia should be distinguished from all dermatosis, manifested by a focal lesion or loss of hair on the head, which occurs against the background of inflammatory skin reaction. Differential diagnosis is determined by the clinical characteristics of the scalp mycosis. In cases where the clinical picture is dominated by peeling with minimal inflammatory skin reaction, the disease should be differentiated with trichophytosis of the scalp, seborrheic dermatitis or psoriasis. In the presence of more pronounced focal hair loss, differential diagnosis should be made with focal alopecia, secondary syphilis.
Smooth skin microsporia is differentiated with eczematid, plaque (numeric) eczema and psoriasis.
Treatment. In case of microsporia of the scalp or multiple rashes on the smooth skin is prescribed inside antifungal antibiotic - griseofulvin. It is assumed that when taken orally, the antibiotic comes from the intestines into the blood, adsorbed by the epidermis cells and accumulates in the stratum corneum and appendages of the skin (hair, nails), all of which become inaccessible to the introduction of the fungus. As the griseofulvin is further applied, the affected part of the hair (or nail) is gradually "pushed out by the growing part". This is why it is recommended to shave the growing hair every 7-10 days with griseofulvin. Griseofulvin is taken in tablets of 0.125 g with meals and drunk 1 teaspoon of sunflower oil or fish oil for better resorption of the preparation in the small intestine. Daily and course doses of the drug depend on body weight and age of the patient, and is 20-22 mg/kg of weight. Treatment with grizeofulvin is carried out under the control of urine and blood tests once in 7-10 days. Griseofulvin is prescribed in 3 doses, for children at the rate of 21-22 mg/kg of body weight per day. The drug is taken daily until the first negative test for fungi. Then in the same dose for 2 weeks after a day and 2 weeks 2 times a week. The first control trial for mushrooms is conducted 10-14 days after the beginning of treatment, the next - 3-4 days before the negative results, then every 5-7 days. (3-fold negative test).
Contraindications: diseases of the liver, kidneys, blood, malignant neoplasms, cerebral circulation disorders, stroke, porphyria (grizeofulvin urgent photosensitization), pregnancy, the period of breastfeeding of the child.
Grizeofulvin can be replaced by imidazole (keto-conazole, nizoral), lamisil or terbisil. Nizoral (keto konazole) is appointed on 1 table (0.2 g) once a day for 2-8 weeks. Terbisil is available in the form of tablets of 125 and 250 mg. Adults are appointed to 125 mg 2 times a day or 250 mg once a day. For children the dose of the drug is set depending on body weight. The duration of treatment with terbisil in mycoses of smooth skin - 2-4 weeks, the scalp - 4-6 weeks.
At the same time, local treatment is also performed. In the course of treatment in patients with scalp microsporia it is necessary to shave the hair weekly, wash the head with water and soap 2 times a week. It is recommended to lubricate the hearths with 2-5 % iodine alcohol solution and rub into the scalp and smooth skin antifungal ointments (Vilkinson ointment, sulfuricyl (10%), sulfuricyl (3%), sulfuric (5%), degty (10%) ointments, mikoseptin, keto-conazole cream, lamisil, clotrimazole, etc.).
Prophylaxis. Prophylactic measures in microsporia include the control of stray cats and veterinary supervision of domestic cats and dogs, as most infections occur from these animals. Given the possibility of infecting children from each other through direct contact, as well as through objects (headdresses, combs, towels), schoolchildren should be examined at least twice a year, before and after summer vacations. Children treated for microsporia may be admitted to children's groups only after three negative results of microscopic check-ups of hair.
Trichophytosis - trichomycosis caused by trichophytons. A distinction is made between surface and infiltration-prone trichophytosis.
The surface trichophytosis is caused by anthropophilic fungi Trichophyton violaceum and Trichopbyton tonsurans. The source of infection is usually adults, usually women suffering from chronic superficial trichophytosis, and children with the manifestation of the disease. Infection occurs through direct contact with the patient or through headgear, bedding, combs, combs, hair clippers and other objects and things used by the patient. Usually mycosis is transmitted in a family with a chronic trichophytosis patient; it may be transmitted in hairdressing salons, kindergartens, boarding schools, schools, and other children's institutions. Surface trichophytosis, a disease of preschool and primary school-age children, is also found in adolescents and adults, usually in women in chronic form. Depending on localization, superficial trichophytosis of the scalp and smooth skin is distinguished. Affection of nails with superficial trichophytosis is less common. Surface trichophytosis of the scalp (tinea capitis) is first characterized by single and then multiple foci with diameters from 1 to 2 cm, usually one of the foci is 3-4 times larger, irregularly shaped, with unclear boundaries. Foci are isolated, with no tendency to merge with each other, the skin in the area of the centers is slightly puffy and hyperemic, covered with branched flakes of silver-white color, the layering of which may give the focus a whitish appearance. Sometimes, hyperemia and swelling increases, bubbles, pustules, crusts join, especially on the periphery. Within the hearths, hair thinning is noted due to its breakage at the level of 2-3 mm from the skin surface or at the root itself, which is much rarer. Cracked hair leaves a stump in the form of a black dot at the mouth of the follicles ("lichen black dots"). Removed hair fragments are often twisted, looking like a hook.
The diagnosis, always requiring laboratory confirmation, is relatively simple.
Differential diagnostics
The characteristic change of hair and poor inflammatory response allows us to distinguish the superficial trichophytosis of the scalp from psoriasis and seborrheic eczema. Differential diagnosis with microsporiasis is possible only with the help of microscopic examination of the affected hair and examination of the child's head under a fluorescent lamp.
Superficial trichophytosis of smooth skin, in particular of the face (Dermatophytny trunk, tinea, corporls) can be isolated or combined with the lesion of the scalp. It is localized mainly on the open areas of the skin: face, neck, forearms, as well as the torso.
Surface trichophytosis of the scalp may be manifested in three clinical forms: erythematoso-vezicular, squamous, and impetiginous.
In erythemato-vezicular form, foci of pale hyperemia and minor edema with relatively clear borders, rounded shape, up to 2.5 cm in diameter, appear on the scalp, mainly in the parietal part. On the surface of the foci appear microvesicular elements, dried up with the formation of layered microcorns, forming in the future fine-plate peeling. The hair is broken at skin level.
Squamous form of surface trichophytosis is the most common. This clinical variety is characterized by areas of skin exfoliation without clear boundaries or signs of inflammation. Hair in the lesions is thickened but easily broken at different levels or directly at the exit point of the hair follicle, forming "black spots". In addition, part of the hair is twisted as a comma. At the same time, it is possible to partially save in the lesion area of the hair of a normal form.
Impethygenetic form of surface trichophytosis of the scalp is characterized by a more pronounced exudation in the lesion area, which leads to the formation of yellowish-colored scales, resembling a vulgar impetigo.
Superficial trichophytosis of smooth skin. Surface trichophytosis of smooth skin occurs more often on the face, neck, hands and forearms, less often any part of the skin can be involved in the process. Foci of lesion, single or multiple, have clear boundaries, rounded or oval disc-shaped. There are two zones that give a similarity to the disk. Peripheral - inflammatory, represented by hyperemia, edema and the formation of papulosis and vesiculosis elements on their surface - rises above the skin level in the form of a roller. The central zone (partial regress) - pale, westerly, covered with finely lamellar scales. In some cases, there is no distinct vesiculation on the surface of the focus, and on the background of erythema flakes appear, bypassing the stage of wetness.
This type of mycotic skin lesion has great clinical resemblance to numeral eczema. This similarity is enhanced by the ability of the centers of superficial trichophytosis of smooth skin to merge with each other, with the formation of extensive areas of lesions with bizarre outlines. The course of dermatosis is initially acute, later it becomes protracted, which is usually associated with additional damage to cannon hair. However, under the influence of rational etiotropic therapy, changes occur within a few days.
Foci are isolated, with no tendency to merge with each other, the skin in the area of the centers is slightly swollen and hyperemic, covered with branched flakes of grayish-white color, layers of which can give the focus a whitish appearance; sometimes the hyperemia and swelling increases, joined by bubbles, pustules, crusts, especially on the periphery. Within the hearths, hair thinning due to hair breakage is observed. Hair is broken at a level of 2-3 mm from the skin surface or at the root itself, which is much less common. The diagnosis, which always requires laboratory confirmation, is relatively simple. The characteristic change of hair and poor inflammatory response can distinguish the surface trichophytic hair of the scalp from psoriasis and seborrheic eczema. Differential diagnosis with microsporiasis is possible only with the help of microscopic examination of the affected hair and examination of the child's head under a fluorescent lamp. Surface trichophytosis of smooth skin can be isolated or combined with the lesion of the scalp. It is localized mainly on the open areas of the skin: face, neck, forearms, as well as the torso. The disease begins with the appearance of one or more oedemas and therefore slightly protruding over the level of the surrounding skin spots of pink and red color, correct rounded outlines, with sharp borders. Their surface is covered with 'flakes' and small bubbles that quickly dry out into crusts. The center of defeat becomes a ring with time. Sometimes, a fresh spot appears on the skin of the surviving center, passing the same development cycle - there are ring-shaped forms included in one another (a symptom of "iris"). The centers of the merged spots have festoon-shaped outlines. Cannon hair in the hearths are affected, often broken, thickened, dull Subjective sensations are expressed in a small itch, sometimes completely absent.
Trichophytosis is chronic in adults, mainly in women (80%), has poor clinical manifestations. In most cases, they are infected with superficial trichophytosis in childhood. Being untreated, the disease lasts for decades without giving any subjective sensations. Chronic trichophytosis occurs exclusively in women, mainly suffering from genital and thyroid hypofunction. In this form, usually first there is a lesion of the scalp, and then there are seats on the smooth skin, involved in the process of skin of the palms and soles, nail plates of the hands and feet.
It should be noted that it may be women who have isolated trichophytosis of the scalp.
Chronic trichophytosis of the scalp has poor symptomatology, because it runs in an erased form. The main clinical symptom is the discovery of comedic "black dots" - hairs that have broken directly at the outlet of the hair follicle. This is a so-called "black spot" form of chronic trichophytosis. It localizes mainly in the occipital region, where, in addition to the broken hair, there is a slight cyanosis and poor branched peeling. Affection of smooth skin in chronic adult trichophytosis, usually localized on the shins, buttocks, forearms, less often on the face and torso, is represented by psoriasiform foci without clear boundaries. Mild hyperemia, superficial infiltration and fine-plate peeling in the central part of the focus may be combined with more pronounced inflammatory changes in the peripheral growth zone or in new small lesions. These fine "dropouts" are the result of cannon hair lesions and give the disease a chronic relapse.
Affection of the palms and soles in chronic trichophytosis is practically not accompanied by inflammatory changes. There is a thickening of the stratum corneum (palm-plate hyperkeratosis), combined with fine lamellar exfoliation, reminiscent of dyshydrotic. Although this form of trichophytosis, unlike dyshydrosis, never produces vesicular elements.
Nail plates are involved in the process almost simultaneously with the skin of the palms and soles.
Trichophytosis of the nails occurs exclusively in adults, and the lesion of almost all the nail plates has a characteristic clinical picture. The change of the nail begins from the external or external-lateral regions with subsequent spread to the sprout zone. The nail plate loses its smoothness, transparency and gloss. It becomes thickened, layered, split at the free edge. These changes are accompanied by footstep hypekeratosis. The nails acquire first a yellowish gray, then a dark brown color. Gradually separating from the nail bed, from the free edge form empty spaces under the nail plate. In the future, it is possible to reject the nail plate, which does not, however, lead to self-healing.
Histopathology. Histopathological picture is different depending on the clinical form of mycosis. In superficial trichophytosis of smooth skin, the corneal layer is loosened, there is para-keratosis, acanthosis and serous inflammation in the malpigial layer, up to the formation of bubbles. In the papillary and hypodermic layers of the dermis, edema, vasodilatation and polymorphic vascular infiltration are determined. Mycelium and fungus spores are found between the horn plates. In chronic trichophytosis of the scalp, the above changes are joined by changes in the follicles and hair. In the follicular and peri-follicular zones, inflammatory phenomena are visible to varying degrees, and the hair is permeated with mycelium threads and filled with spores.
Differential diagnostics
The diagnosis is made on the basis of the clinical picture, the results of laboratory tests (endotrix hair lesion, fungus elements in skin scales, nail particles, excretion of the culture of the pathogen), epidemiological history (contact with patients).
Differentiated from microsporia, skin lesions caused by Trbrum, favaea, microbial and seborrheic eczema, pink sheepskin, inguinal epidermophy.
Treatment: Inside prescription of one of the antimicrobial antibiotics: grizeofulvin, nizorul, orungal, terbisil (see microsporia).
Local: fungicidal solutions and ointments. Hair is shaved.
Prevention - identification of patients with chronic trichophytosis of the scalp.
Infiltrative-negative or zoophilic trichophytosis.
Previously, this form, caused by zoanthropophilic fungi, was called deep trichophytosis (Tr.profiindus), because it was characterized by the formation of deep suppurative nodes. At present, it has been established that zoanthropophilic fungi in humans can cause a clinical picture with varying degrees of inflammation. When diagnosing trichophytosis, it is recommended not to limit ourselves to microscopy (to confirm the fungal nature of the disease), but to produce a bacteriological (cultural) study to determine the type of pathogen, which is of great epidemiological importance.
Infiltrative-forecasting trichophytosis is mainly caused by Trichophyton verrucosum and Trichophyton raentagrophytes var. gypseum.
In some regions of our country, patients with this form of trichophytosis account for more than 50% of all patients with surface trichophytosis, microsporia and favaux combined. At the same time, the role of gypsum trichophyton is increasing in comparison with faviform trichophyton.
Human infection occurs in contact with animals with trichophytosis or with objects infected by these pathogens. Sick animals serve as a source of infection, less often - a sick person. An epidemic chain is possible: mice - cattle - human. Usually, the pathogens parasitize on rodents, including laboratory ones - under Tg. gypseum, less often on cows, calves, horses, sheep - under Tg. verrucosum. Infiltrative-negative trichophytosis often acts as an occupational disease, especially in cattle breeders, workers with fur beasts (mink, sable, foxes, etc.).
In the epidemiology of this trichophytosis, except for animals, which have already been mentioned, pay attention to the insects (fungi carriers), as well as the possibility of developing zoanthropophilus fungi in straw, corn stems. The role of soil in the cycle of development, conservation (reservoir) and transmission of zoophilic dermatophytes and the issue of mykonosynthesis of zoophilic trichophytes among animals are intensively studied. Contribute to the infection of micro-traumas, the duration and massiveness of healthy human contact with infectious material, virulence of pathogen strains, the state of reactivity of the body, often determining the shape and course of mycosis.
Clinically infiltrative and predictive trichophytosis is characterized by sharply pronounced inflammatory phenomena, often reaching the stage of purulence, and short (up to 2-3 months) cyclic course, ending in complete recovery without a tendency to relapse. The process may involve smooth skin (usually open areas), scalp, beard and mustache area (parasitic sycose). With the development of suppuration, the hearths acquire the appearance of the most typical for infiltrative-forecasting trichophytosis. On the scalp, beard and mustache area, they are sharply delineated hemispherical or flattened nodes of blue-red color, lumpy surface of which is covered with osteopolliculites, erosions, and sometimes ulceration, crusts and scales. Some of the hair falls out, some of it is loosened and easily removed. A characteristic feature is the sharply dilated mouths of hair follicles, filled with pus that stands out when pressed in the form of abundant droplets and even pods. At first, the dense consistency of the nodes becomes soft and doughy with time. These centers on the scalp resemble honeycomb (kerion Celsi), and in the beard and mustache area - wine berries. In some cases, the appearance of secondary rashes such as erythema (bark-shaped or scarlet-like), follicular nodules (trichophytes) is observed.
Infiltration and prediction trichophytosis of smooth skin is less acute. Flat plaques prevail, sometimes very large, with isolated papules on the surface, transformed gradually into pustule elements. Consistently, the pustules open up and the released pus dries up to form brownish-greenish crusts. The developed purulence causes the death of mushrooms. They are preserved only in scales at the periphery of the lesion centers, where they are found during microscopic examination.
Histopathology. Intrafollicular abscesses and perifolliculites containing neutrophilic and eosinophilic granulocytes are detected, followed by single giant cells. The abscess cavities are filled with granulation cloth with epithelium and giant cells. The mushrooms are found in the epidermis and even in the granulomas.
The outcome of the disease is scar formation. As a result of strong immunity that occurs in infiltrative-negative trichophytosis, there are no relapses.
The diagnosis is based on the clinical picture, the results of microscopic and cultural studies.
Differential diagnosis of infiltration-normative trichophytosis is made with an infiltration-normative form of microsporia. The latter is caused by a fluffy microsporium and is relatively rare. In case of localization of foci on the skin, the lesion in men is differentiated from vulgar (staphylococcus) sycotism, which usually takes a long time, without a pronounced inflammatory phenomena. The follicular nature of the lesion and the acute course of the process allow us to distinguish zoophilic trichophytosis from chronic pyodermia and deep mycosis (sporotrichosis, deep blastomycosis, etc.).
Treatment: sanation of the affected hair, without which it is impossible to fully cure and prevent relapses. Appointment of grize-ofulvin and nizoral inside. Daily dose of grizeofulvin in all forms of trichophytosis is determined at the rate of 16 mg per 1 kg of patient's body weight. In this dose the preparation is taken daily until the first negative microscopic examination for the presence of fungi, which usually takes 3-4 weeks, then 2 weeks after a day and then another 2 weeks once in 3 days. Treatment is considered to be complete with three negative results of the study, conducted at intervals of 5-7 days. Terbysil is prescribed to adults and adolescents for 250 mg (1 tablet) per day, to young children up to 125 mg. The duration of treatment is up to 2-3 months. Criteria cured the same as in the treatment with griseofulvin. Hair in the areas of lesions on the head shaved once a week. Local treatment is to lubricate smooth skin and scalp with 2-5% iodine alcohol solution in the morning and micozolone in the evening. Sulphuric (10%)-salicyl (3%), sulfur (5%)-degtyar (10%) ointments and Wilkinson ointment are used. With sporadic foci on smooth skin, treatment is limited to external remedies with obligatory removal of cannon hair with epilation tweezers.
Prevention of zoonotic trichophytosis is mainly focused on the identification and treatment of sick animals and deratization; these activities are implemented in conjunction with the veterinary service.
Favus (syn.: parsley, tinea favosa, tinea lupinosa, trichophytia fa-vosa) - chronic fungal disease of skin, hair, nails and sometimes internal organs. Without treatment, the disease lasts for years and decades. There are cases when the patients suffered from fava from early childhood to deep old age.
The disease is more common in Europe, Asia, and North America. In Russia, it is registered in isolated cases.
Etiology. Favus causative agent was discovered by Remak in 1837, and its fungal nature was established by Schonlein in 1839.
According to modern ideas of the pathogens of the disease belong to the genus Trichophytes. Among them are anthropophiles - Tr. schonleinii (Ashorion schonleinii), which affects people, and zoophytes - Tr . Zopf, affecting cats, mice, dogs, birds, horses, less often - human.
The causative agent of human fauna, unlike others, does not have persistent virulence and contagiousness. Despite the close contact of patients with healthy ones in the family and school, not everyone gets sick. If there is a sick person in the family, the "chain" of infection lasts for years at intervals of several years. This is due to the features of the fungus itself, the dynamics of its pathogenicity, as well as the conditions of its introduction and reproduction in the skin. There is evidence that the faunus causative agent in affected and fallen hair can live for years. This dictates the need to constantly carry out sanitary and epidemiological measures in the focus of infection before its elimination. However, long and close contact is necessary for transmission. Both the patient himself and his household items (clothes, hats, fur collars, combs, toys, bed linen) are dangerous. Therefore, the disease, as a rule, has the character of family centers. Favusom is more often infected by children, but often also by adults, who are the main source of infection. And usually the infection is transmitted through the female line.
Factors predisposing to the development of favus are conditionally divided into two groups - exogenous and endogenous. The first group mainly leads to a disturbance of the physiological barrier (protective) function of the skin. These include, first of all, superficial and deep injuries with violation of epidermis integrity. Endogenous factors lead to a decrease in the general resistant organism and its resistance to infection. Among the latter, endocrinopathies, hypovitaminosis, intoxications, concomitant chronic diseases, immunodeficiency states, etc. are of great importance. It is necessary to take into account such iatrogenic effects as taking glucocorticoid hormones, immunosuppressive and cytostatic drugs.
The incubation period in favaux is 2-3 weeks.
The lesion of the scalp is characterized by three clinical signs:
- the formation of a specific favaux, the so-called shield - cheekbones, which is a pure mushroom culture;
- hair affection with subsequent loss (in case of other fungal diseases, the hair breaks down);
- development in places where scar atrophy of the skin is affected, leading to persistent alopecia.
The clinical picture of the faunus flow was described by Remark, who instilled this infection. After penetration of the fawus agent into the skin, and germinating, it produces a powerful and compact plexus that penetrates the mouth of the hair follicle. Clinically, on the 14th day after infection, a bright red spot appears around the hair with flaking on the surface, accompanied by itching. At the mouth of the hair follicle, a translucent yellow pustule appears, which represents the initial stage of cheekbone formation. Subsequently, the cheekbones take the form of dry crusts of bright yellow color, from which the hair comes out. At the place of their exit, there is a west. The cheekbones gradually increase in size, reaching 1.5 cm in diameter, and take a saucer-shaped shape. Their color becomes grayish-yellow, sometimes with a greenish or brownish tint. The cheekbones are surrounded by a narrow, pink inflammatory rim. Without treatment, the cheekbones merge with the formation of solid crusts, reminiscent of sealed honeycomb (hence the name of the disease: favus-cells). They emit a "mouse" (stale, barn) smell, which arises from the metabolites of the accompanying microbial flora. Erosion with a smooth, wet bottom of a bright red color is formed when the crusts are removed.
Hair damage occurs through the penetration of the fungus in both the root and rod parts. The hair loses its shine, becomes lifeless, dull, dry and gets a grayish-white color. In contrast to the damage of the hair in trichophytosis and microsporia, they do not break, but fall out entirely or remain soluble in the thickness of the cheekbone. In the latter case, the hair protrudes in different directions, like a bag, reminiscent of a wig (favorite).
The third characteristic feature of lousy hair, especially in the long run, is skin atrophy, first nesting, in place of the cheekbones, and later diffuse and almost solid. The skin in the scars area is thin, smooth and shiny. The hair follicles are destroyed, resulting in persistent alopecia.
Along with the typical scutular form of lousy, there are squamous (pitiriaziform) and impetrigenous types of lesions on the scalp. The squamous form is characterized by the appearance of small or large scales of grayish-white color, pierced with dull hair. The cheekbones are either absent or small, dotted. Atrophy and persistent alopecia are formed at the place of process resolution. In case of impetrigenous form, the lesions are also formed in the mouths of hair follicles. They are pustules, the contents of which, when dried, form massive dry yellow crusts that resemble hypetiginal. Typical hair changes, alopecia and atrophy of the skin are also characteristic of this form.
The faveus of smooth skin is found on open and closed parts of the body - on the face, neck, extremities. At the beginning, small spots appear on the skin with small bubbles appearing on the periphery and sitting on a tight base. In place of the opened bubbles, as a result of the drying of exudate, yellow crusts are formed, tightly soldered with the skin. Gradually, they acquire the appearance of typical skulls. As a result of the appearance of fresh elements and their fusion, there is the formation of extensive centers of lesions. Foci, as a rule, are located in separate areas, but universal defeat is possible. At the resolution of rashes on the smooth skin of the scar atrophy is not left. Sometimes, the defeat of smooth skin is atypical in the form of the appearance of limited, slightly infiltrated spots of pink with peeling on the surface, more clearly expressed in the area of hair follicles.
The affected nail plates thicken, lose their luster, become bumpy, germinate with yellow sculls and crumble. Usually the nails of the fingers are affected, less often the feet.
Diagnostics
Microscopic examination
Pathological material is taken from the lesion area - scales of skin, hair, nails. For preparation of preparations the material is crushed using a scalpel. For a clearer identification of the elements of the fungus produce enlightenment (maceration) of the material To this end, the material is placed in a solution of caustic alkali (KON, NaOH) 20-30 %. The alkali dissolves the epidermal scales, mucus, pus, enlightens the hair pigment. This makes the mushrooms available for research. After heating over a flame, the material is tested within 2 hours from the moment of preparation. Being in the hair, the mushroom is polymorphic: chains of spores in the form of threads and clusters, air bubbles and fat drops.
The cultural study is a highly sensitive and specific method of laboratory diagnostics. It makes it possible to determine the genus and type of causative agent. Saburo or wort agar is used for sowing. Sowing is incubated at 28 ° C, growth of dermatophytes begins on the 4th to 12th day of incubation. No growth for 30 days is considered a negative result.
The luminescent method is used to diagnose the fava. In the ultraviolet rays passed through the Voodoo filter, the completely affected hair glow with its characteristic greenish color. This method is also used to monitor the effectiveness of the treatment. The examination is carried out in a darkened room, the lesions must first be cleaned of crusts and ointment residues.
Differential diagnostics of the scalp faunus is carried out with other mycoses.
In microsporia, lesions are few (1-2), rounded, with noticeable inflammatory infiltration, densely covered with grayish-white, sometimes asbestos-like scales. Hair breaks at 4-8 mm and looks short cut. Broken hair has a grayish-white color due to a mushroom spore cover. Hair can be pulled out easily along the edge of the hair centers. There is a green glow in the rays of Vood.
Foci of superficial trichophythia have irregular rounded shape, blurred borders, are characterized by weak hyperemia and slight flaking. An important symptom is the thinning of the hair, which is not caused by loss, but their breakage at different levels. Some hair breaks at a height of 2-3 mm, others - at the exit from the mouth of the hair follicle, taking the form of black spots.
In chronic "black spot" trichophytic hair part of the head is located in the occipital and temporal regions, where there is a slight branched peeling. Pathognomonic symptoms are black spots due to hair breakage at skin level. Their number may vary from singular to multiple.
Differential diagnosis of the fauna of smooth skin is carried out with superficial and chronic trichophytosis, as well as with microsporia" The clinical manifestations of superficial trichophytosis and microsporia of smooth skin are very similar. The primary morphological element of the skin rash is one or more spots with clear borders, slightly elevated above the skin level. They are prone to centrifugal growth. They distinctly distinguish the two zones. Peripheral - in the form of a rising rim of inflamed skin covered with small nodules, bubbles and crusts. Central - pale pink with branched peeling, in the area of which occurs the reverse development of the spot (self-resolution). As the peripheral growth and the simultaneous central resolution, the elements take on the form of rings. In the center, due to autoinoculation of the pathogen a new focus is formed and a "ring in the ring" appears. Smooth skin microsports are usually characterized by multiple centers.
In chronic trichophytosis, skin areas subject to friction and maceration are affected. Foci are peeling pinkish-violet spots with blurred borders. They do not tend to have a central resolution. But nodules in the form of rings may appear on their background.
The principles of treatment of fava do not differ from those generally accepted in mycology. After confirmation of the diagnosis, the patients with fa fava are isolated. Examination of persons in contact is carried out once in 10 days during 1 month, then in 3, 6 and 12 months, then - once a year for 5 years. Hospitalization of patients is carried out in case of lesion of the scalp or when the skin has more than 2, 3 foci. For treatment they use grizeofupvine at the rate of 17 mg/kg of body weight in combination with local antifungal (5% p-p of iodine, fungicide ointments). Treatment with lamisilom, terbisil by cxeMef trichophytosis is possible. The patient may be discharged from the hospital after 3 negative tests at intervals of 5-7 days. After the end of treatment patients with fava are registered for the 1st year, with the examination in the 1st month weekly, the second and third - once a month, then -1 time per quarter. In foci of disease incidence, repeated examinations of patients are carried out annually for 5 years.
Prophylaxis
Control of family and other hearths once a month in the first quarter and then annually for 5 years. After the control surveillance, patients are removed from the register in case if during this period of time there were no identified sick people. In addition, disinfection measures are taken in foci.
Dermatomycoses - HIV markers
Common fungal lesions of the skin and nail plates caused by dermatophytes are relatively common with HIV infection. Diseases can occur in the form of typical dermatomycosis lesions of the skin of feet, hands, shins and other parts of the body, as well as atypically.
Atypical manifestations of dermatomycosis in AIDS patients usually occur on the face and neck and may resemble erythema, seborrheic dermatitis, folliculitis. "Rubrophythia" in the palms and soles often shows signs of palm-sole or gonorrheic keratodermia. Onyhomycosis in AIDS patients occur in isolation or in combination with lesions of the palms and soles. Their cause is most often red trichophyton. A characteristic feature of these onychomycoses is the frequent development of paroniasis.
Mycotic skin lesions
They are usually caused by red trichophyton, and the hearths of rubrophythia are multiple and extensive.
Sometimes there is an inguinal epidermofitiya, which can go beyond its usual localization and affect the body, hands, feet and even face.
It is heavy, poorly treatable, and repeats the colorful (branched) lichen.
Candidosis of the skin and mucous membranes is most common in AIDS. It is characterized by the young age of patients, predominant lesions of the mucous membranes of the mouth, esophagus, genitals and perioral region, a propensity for erosion and ulceration, relapse, resistance to therapy.
Cryptococcosis
Since extrapulmonary forms of cryptococcosis are among AIDS-infectious diseases, timely recognition of this little-known mycosis in our country is essential for early diagnosis of HIV infection.
Rashes often resemble herpes, so suspicious lesions should be examined for the presence of pathogens (virus secretion, fluorescent antibody method) or histologically diagnosed. Described by an AIDS patient who has papules on his face that resemble an infectious mollusk. In a cultural study of skin and cerebrospinal fluid, Cryptococcus neoformas yeast fungi were identified.
Skin changes in Cryptococcus may also occur as panniculitis, vasculitis, subcutaneous abscesses, ulcers, vegetating papules, folliculitis. If cryptococcosis of the skin, the patient should be carefully examined to detect a disseminated process (it is recommended to examine for cryptococcosis sputum, saliva, urine, prostatic juice), because the skin symptoms may precede systemic manifestations of mycosis, especially lesions of the nervous system and lungs.
Diagnosis of cryptococcosis is based on the discovery of characteristic round or oval yeast cells with a wide capsule in biopsy tissues. In histological preparations, renal cells are often seen. Similar fungal elements are found in cultures of the causative agent. A reliable laboratory method is also the detection of cryptococcal antigen directly in tissues by indirect immunofluorescence or immuno-peroxidase technique, as well as in various biological fluids (urine, cerebrospinal fluid), using the latex agglutination reaction and immunoassay.
Amphotericin B (administered slowly intravenously in glucose solution at the rate of 0.1-0.5 mg/kg in gradually increasing doses) and 5-fluorocytosine (orally or intravenously 100-150 mg/kg 3-4 times a day for 5-6 weeks) are used for treatment of cryptococcosis patients. Long-term treatment, after cessation of antifungal drugs is often observed relapses or reinfections, so in some cases, use the prophylactic administration of myconazole drugs (eg, ketoconazole 0.2-0.4 g 2 times a day by oral) or 5-fluorocytosine.
Skin histoplasmosis
This is a relatively rare complication of AIDS, although histoplasmosis is fairly common in endemic areas (USA, Africa). In any case, this mycosis is one of the 12 AIDS-infected diseases with laboratory confirmation of HIV infection. Skin manifestations are not specific. Discrete papules have been described along the edge of the palms and soles, with keratotic plugs in the center of these papules. A histological study of skin lesions revealed granulomatous infiltration with a large number of tissue forms of the causative agent - histoplasmosis is caused by dimorphic mushrooms with mycelial cultural and yeast tissue forms. Other skin manifestations of histoplasmosis are folliculitis, pustules, papulo-necrotic foci, perianal ulcers, spotty-papuloid rash with peeling. The diagnosis should be confirmed by histological or cytological, as well as cultural study of lesions. In Saburo agar with glucose, cultures with characteristic "spiky" macroconidia are distinguished, and in blood agar at 37 ° C - yeast forms of the pathogen.
By: Dr. Cindy Li